
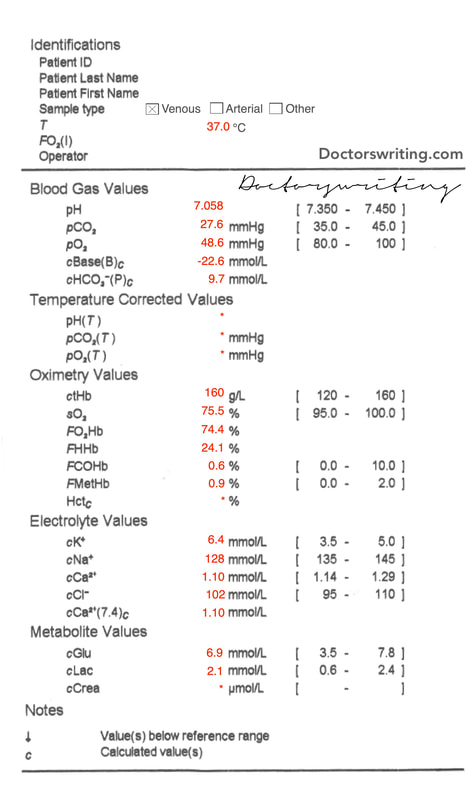
 | A 55 year old female is brought to your ED with dyspnoea and fatigue. A venous gas is performed... |
For a basic approach to blood gas interpretation see here
1. What is the Acid-Base disturbance?
pH = 7.058 ∴ severe acidosis
Cause of acidosis?
Is there appropriate respiratory compensation or a concomitant process?
What is the cause of the metabolic acidosis?
If you want to be pedantic and call it a HAGMA - then we can check if there is another concomitant metabolic process:
Cause of acidosis?
- CO2 = 27.6 ∴ primary metabolic acidosis
Is there appropriate respiratory compensation or a concomitant process?
- Expected CO2 = 1.5 x HCO3 + 8 = 22.55
- Actual CO2 = 27.6 ∴ concomitant mild respiratory acidosis
What is the cause of the metabolic acidosis?
- Anion Gap = 128 - 102 - 9.7 = 16.3 = NAGMA (well...normal is 12 +/- 4 🤷♂️)
If you want to be pedantic and call it a HAGMA - then we can check if there is another concomitant metabolic process:
- Delta Ratio = (16.3 - 12) / (24 - 9.7) = 0.3
- DR < 0.4 so this is a hyperchloraemic NAGMA
2. Are there any electrolyte issues?
Na (for glc)
K (for pH)
Ca (for alb)
- Since Glc is normal, we don't really need to check - we know its hyponatraemia
- Actual Na - mNa + (Glc - 5)/3 = 128 + (6.9 - 5)/3 = 128.8
- ∴ Hyponatraemic
K (for pH)
- Expected K = 5(7.4 - pH) +5 = 5(7.4 - 7.058) + 5 = 6.71
- Actual K = 6.4 ∴ Essentially normal K
Ca (for alb)
- Ca = 1.10 and unable to correct as albumin not known
3. Are there any oxygenation issues?
This is a venous sample ∴ unable to calculate
4. Are there any other abnormalities?
COHb & MetHb normal
5. What is your overall impression?
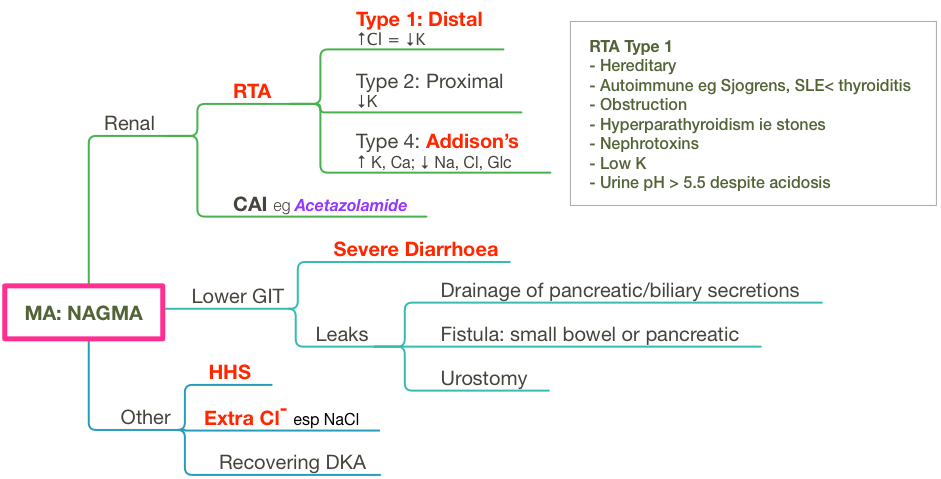
The combination of a Hyperchloraemic NAGMA and those electrolyte abnormalities (specifically high K, low Na & Cl, borderline Glc) suggests Type 4 renal tubular acidosis (see below for the ddx of NAGMA).
The Creatinine was unavailable at the time of the venous gas analysis. It eventually came back as Crea = 890. Further information also revealed that she was on long term steroids and fits with the suspected diagnosis on this gas of an Addisonian picture.
Note that other types of renal failure (ie renal damage affect both tubules AND glomeruli) often cause a HAGMA (at the very least, not a hyperchloraemic NAGMA)
Remember the other types of RTA?
Type 1: Distal aka 'Classic'
Type 2: Proximal
Type 3: Retired
Type 4: Tubular Hyperkalaemia
The Creatinine was unavailable at the time of the venous gas analysis. It eventually came back as Crea = 890. Further information also revealed that she was on long term steroids and fits with the suspected diagnosis on this gas of an Addisonian picture.
Note that other types of renal failure (ie renal damage affect both tubules AND glomeruli) often cause a HAGMA (at the very least, not a hyperchloraemic NAGMA)
Remember the other types of RTA?
Type 1: Distal aka 'Classic'
- Due to inability to secrete H+ = cant acidify urine
- Causes: plenty - see mind map below
- Ix: high Cl, urine pH > 5.5 (despite acidosis), renal stones common, low K later (from 2ry hyperaldosteronism)
- Tx: NaHCO3 (Na + K citrate solutions if low K)
Type 2: Proximal
- Due to impaired HCO3 reabsorption
- Causes: hereditary most common, vit D def, Pb nephropathy, amyloid...other House MD type stuff
- Ix: less severe acidosis, plasma HCO3 > 15, urinary HCO3 +++, low K
- Tx: treat underlying cause, thiazide diuretics
Type 3: Retired
Type 4: Tubular Hyperkalaemia
- Due to renal failure = high plasma K ALWAYS
- Causes: Aldosterone deficiency or resistance
(other acid-base mind maps at the bottom of this page)
 RSS Feed
RSS Feed