
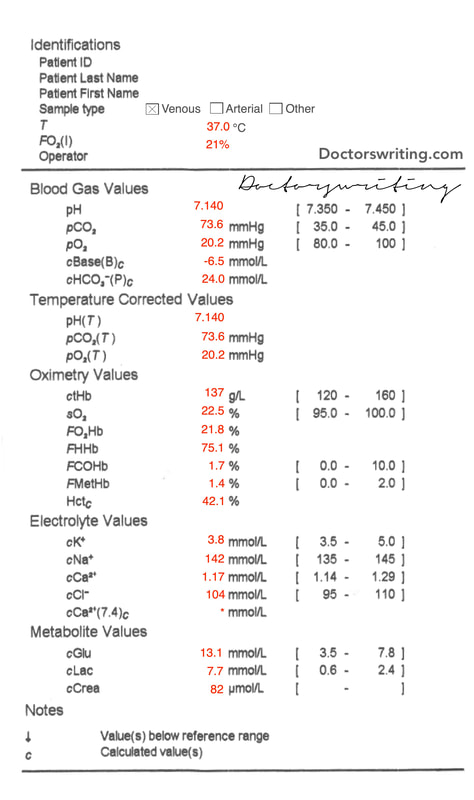
 | 19yo male is brought in by ambulance after being found semi-conscious (P in AVPU) in a parked car. His conscious state improved to "V" on arrival but was starting to regress. A blood gas is performed |
For a basic approach to blood gas interpretation see here
1. What is the Acid-Base disturbance?
pH = 7.140 ∴ moderate acidosis
Cause of acidosis?
Is there appropriate metabolic compensation or a concomitant process?
What type of metabolic acidosis is it?
Overall: Primary respiratory acidosis with partial metabolic compensation (ie metabolic acidosis)
Cause of acidosis?
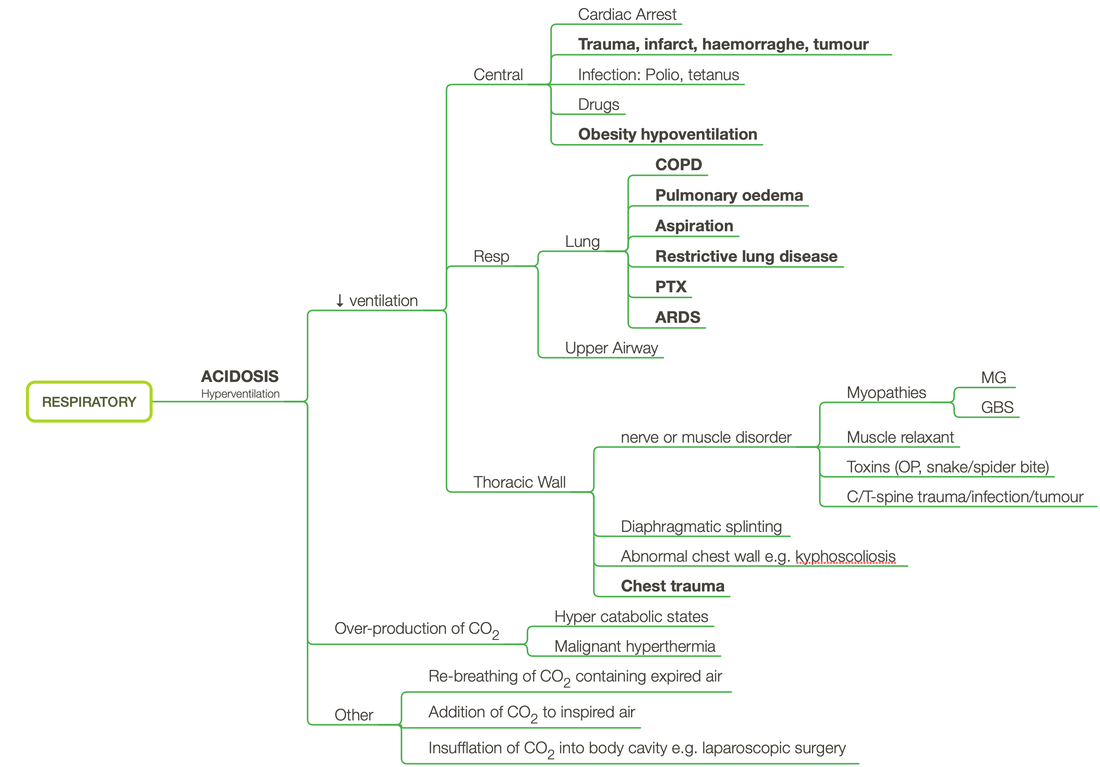
- pCO2 = 73.6 ∴ Primary respiratory acidosis
Is there appropriate metabolic compensation or a concomitant process?
- HCO3 = 24 + 0.1(CO2 - 40) = 24 + 0.1(73.6 - 40) = 27.36
- Actual HCO3 = 24.0 ∴ 𝛥HCO3 = - 3.36 ∴ Concomitant metabolic acidosis
What type of metabolic acidosis is it?
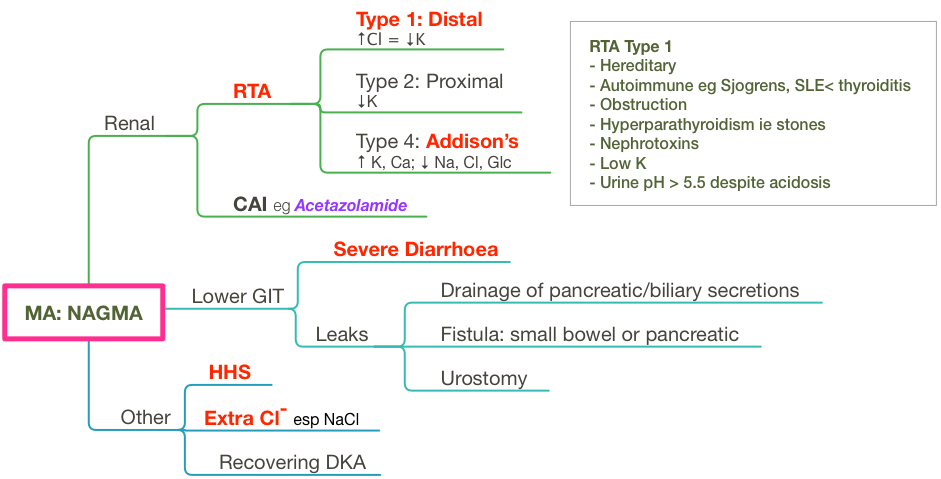
- Anion Gap = 142 - 24 - 104 = 14 ∴ NAGMA
Overall: Primary respiratory acidosis with partial metabolic compensation (ie metabolic acidosis)
2. Are there any electrolyte issues?
Na (for glc)
K (for pH)
Ca (for alb)
Cl (no correction req)
- Actual Na - mNa + (Glc - 5)/3 = 142 + (13.1 - 5)/3 = 144.7 ∴ Normonatraemic
K (for pH)
- Expected K = 5(7.4 - pH) + 5 = 5(7.4 - 7.140) + 5 = 6.3
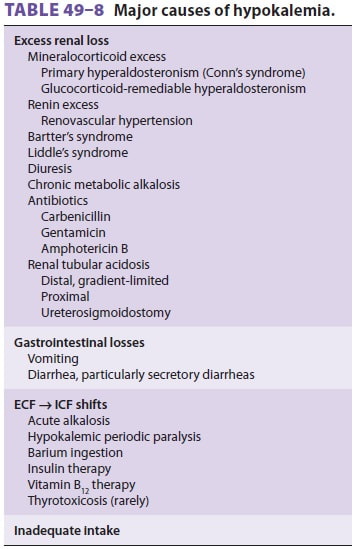
- Actual K = 3.8 ∴ 𝛥K = -2.5 ∴ Severe Hypokalaemia
Ca (for alb)
- CorrCa = 1.17 ∴ Normocalcaemic
Cl (no correction req)
- Cl = 104 ∴ Normochloraemic
3. Are there any oxygenation issues?
This is a venous sample ∴ unable to calculate
4. Are there any other abnormalities?
Lactate high
Glc high
Hb normal
COHb normal
MetHb normal
Glc high
Hb normal
COHb normal
MetHb normal
5. What is your overall impression?
Primary respiratory acidosis with concomitant metabolic acidosis and associated severe hypokalaemia
Respiratory acidosis: given age, likely due to drug-induced respiratory depression ∴ look for other features of tox as well as other causes of altered level of consciousness (esp trauma)
Metabolic acidosis: You would assume that this was due to lactic acidosis - however LA should give you a RAGMA and not a NAGMA. In the context of severe hypokalaemia, it is worth considering RTA type 1 & 2, severe diarrhoea or recovering DKA given the high-ish BSL - further hx & ex is worth considering if the metabolic acidosis does not improve with correcting the primary respiratory acidosis.
Cause of hypokalaemia unclear - consider vomiting as main cause in this presentation
Respiratory acidosis: given age, likely due to drug-induced respiratory depression ∴ look for other features of tox as well as other causes of altered level of consciousness (esp trauma)
Metabolic acidosis: You would assume that this was due to lactic acidosis - however LA should give you a RAGMA and not a NAGMA. In the context of severe hypokalaemia, it is worth considering RTA type 1 & 2, severe diarrhoea or recovering DKA given the high-ish BSL - further hx & ex is worth considering if the metabolic acidosis does not improve with correcting the primary respiratory acidosis.
Cause of hypokalaemia unclear - consider vomiting as main cause in this presentation
|
|
 RSS Feed
RSS Feed