
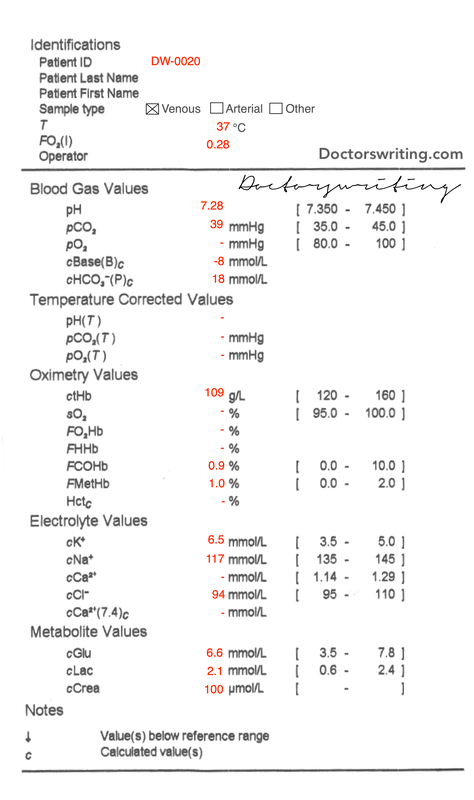
 | A 60 year old male is brought in by ambulance with dyspnoea, falls and low back pain over the last few weeks. His vital signs are normal. A VBG is performed... |
For a basic approach to blood gas interpretation see here
1. What is the Acid-Base disturbance?
pH = 7.28 ∴ moderate acidaemia
Cause of acidosis?
Is there appropriate respiratory compensation or a concomitant respiratory acidosis?
What type of metabolic acidosis is it?
Overall: Primary Low Anion Gap Metabolic Acidosis with partial respiratory compensation
Cause of acidosis?
- HCO3 = 18 (ie < 24) ∴ metabolic
Is there appropriate respiratory compensation or a concomitant respiratory acidosis?
- Expected CO2 (pH < 7.4) = 1.5 x HCO3 + 8 = 1.5 x 18 + 8 = 35
- Actual CO2 = 39.0 ∴ 𝛥CO2 = - 4 ∴ Concomitant respiratory acidosis
What type of metabolic acidosis is it?
- Anion Gap = 117 - 18 - 94 = 5 = LAGMA
Overall: Primary Low Anion Gap Metabolic Acidosis with partial respiratory compensation
2. Are there any electrolyte issues?
Na (for glc)
K (for pH)
Ca (for alb)
Cl (no correction req)
The combination of hyponatraemia and hyperkalaemia is always concerning for hypoadrenocorticism (ie Addison's)
- Actual Na = mNa + (Glc - 5)/3 = 117 + (6.6 - 5)/3 = 117.5 ∴ Severe hypOnatraemia
K (for pH)
- Expected K = 5(7.4 - pH) + 5 = 5(7.4 - 7.28) + 5 = 5.6
- Actual K = 6.5 ∴ 𝛥K = 0.9 ∴ Severe plasma hypERkalaemia (mild total body hypERkalaemia)
Ca (for alb)
- No albumin level to correct to
Cl (no correction req)
- Cl = 94 ∴ severe hypOchloraemia
The combination of hyponatraemia and hyperkalaemia is always concerning for hypoadrenocorticism (ie Addison's)
3. Are there any oxygenation issues?
This is a venous sample ∴ unable to calculate
4. Are there any other abnormalities?
Lactate high
Glc normal
Hb mild anaemia
Crea mildly elevated
COHb normal
MetHb normal
Glc normal
Hb mild anaemia
Crea mildly elevated
COHb normal
MetHb normal
5. What is your overall impression?
Primary Low Anion Gap Metabolic Acidosis with partial respiratory compensation with severe HypOnatraemia, severe plasma HypERkalaemia and HypOchloraemia.
The caveat to LAGMA is the fact that often it highlights one of the limitations of the bedside AG calculation.
Most causes of LAGMA are due to 'unmeasured anions and/or cations'. If this is the case there may in fact be a NAGMA or HAGMA that we're not seeing.
Most of these unmeasured anions/cations are measured with routine bloods (albumin, Ca, Mg) aside from a few exceptions: Bromide overdose (Cl will be falsely elevated), IgG paraprotein in multiple myeloma, lithium and polymixin B.
So where to from here?
Investigating LAGMA
Order your usual panel of 'sick patient' bloods which will include Alb, Ca, Mg and a proper Anion Gap!
The ddx for the ones that this wont pick up can be ruled out or investigated further:
So what did the bloods show?
The caveat to LAGMA is the fact that often it highlights one of the limitations of the bedside AG calculation.
Most causes of LAGMA are due to 'unmeasured anions and/or cations'. If this is the case there may in fact be a NAGMA or HAGMA that we're not seeing.
Most of these unmeasured anions/cations are measured with routine bloods (albumin, Ca, Mg) aside from a few exceptions: Bromide overdose (Cl will be falsely elevated), IgG paraprotein in multiple myeloma, lithium and polymixin B.
So where to from here?
- Seek & Treat the life threats ie is the K+ significant (do an ECG), have a plan for seizures and other complications related to low Na+ and how to correct to minimise iatrogenic injury
- Investigate cause of LAGMA (see below)
- Investigate cause of low Na
Investigating LAGMA
Order your usual panel of 'sick patient' bloods which will include Alb, Ca, Mg and a proper Anion Gap!
The ddx for the ones that this wont pick up can be ruled out or investigated further:
- Bromide OD - chloride isnt elevated
- Multiple myeloma - Full Blood Count will help rule in/out
- Lithium - no medication history or self harm concerns, but can add a level if no luck elsewhere
- Polymixin B - no medication history or self harm concerns
So what did the bloods show?
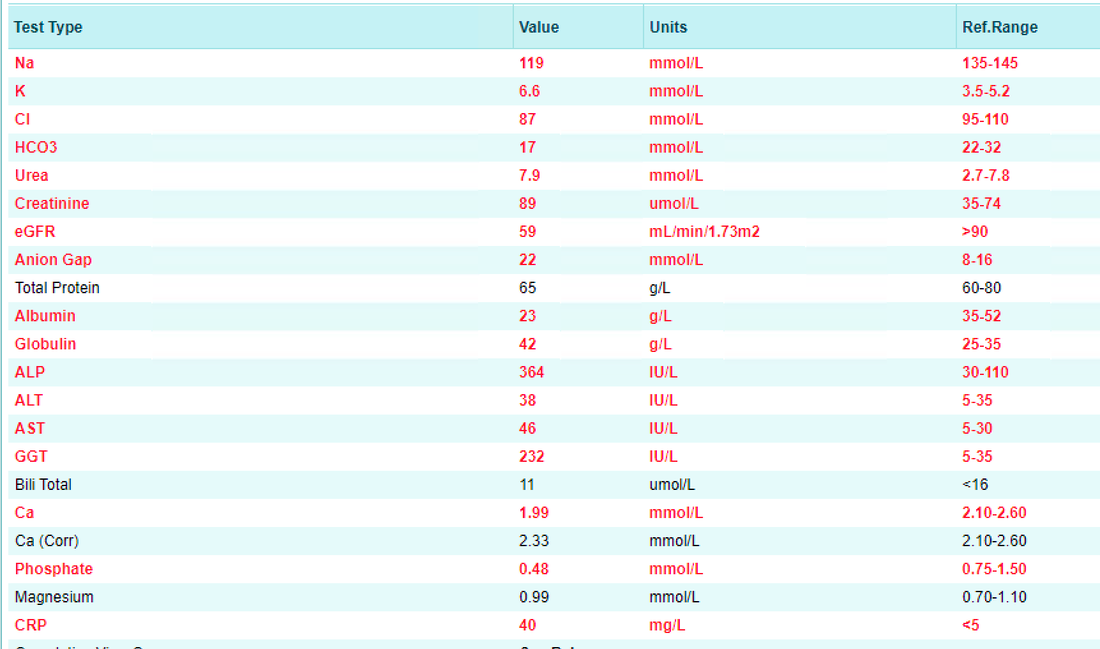
A few thing stand out:
Wait...the Anion Gap is high?!
Lets recap - so our original rule-of-thumb equation for the venous gas was:
So now we have a HAGMA - we should check if this is a true HAGMA, pseudo-HAGMA or mixed N/HAGMA:
And a recap for some of the possibilities for HAGMA (note that Addison's is a NAGMA):
- Albumin is low - which could cause the LAGMA (reduced unmeasured anions)
- Ca & Mg are not the cause of the LAGMA
- The Anion Gap is high! (FYI our lab uses the old style flame photometry to measure this)
Wait...the Anion Gap is high?!
Lets recap - so our original rule-of-thumb equation for the venous gas was:
- Anion Gap = 117 - 18 - 94 = 5
- The AG for the formal eLFTs = 119 - 17 - 87 = 15
- The 'normal' range for AG = 12 +/- 4 ∴ one could assume that this is actually a NAGMA
- However! The 'normal' range for the AG is based on normal values for Alb & PO4
- To corrected the 'normal' AG for patients with deranged Alb and/or PO4 we need to use:
- Corrected normal AG = 0.2 x Alb (g/L) + 1.5 x PO4 (mmol/L) = 0.2 x 23 + 1.5 x 0.48 = 5.3
- Since this patient has a calculated AG of 15, and a normal AG for this patient is 5.3, the patient actually has a severe HAGMA (and it also partially explains the initial ddx of LAGMA)
So now we have a HAGMA - we should check if this is a true HAGMA, pseudo-HAGMA or mixed N/HAGMA:
- Delta Ratio = [AG - 12] / [24 - HCO3] = [22-12]/[24-17] = 1.4 = HAGMA only
And a recap for some of the possibilities for HAGMA (note that Addison's is a NAGMA):
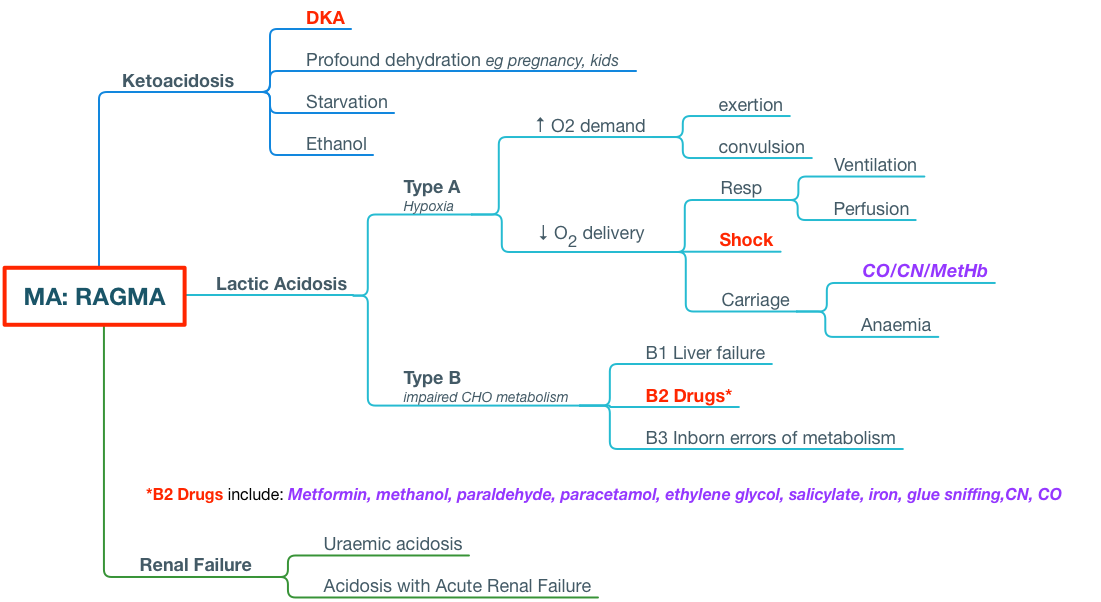
More detective work is needed!
 RSS Feed
RSS Feed