
 | Tom Fuller & Viet Tran The Case A 61 yo female is brought in with a 19 hr history of worsening SOB that suddenly become profound thus prompting an ambulance call. Theres no history of chest pain and no past history of cardiac or respiratory disease that you can elucidate through her short gasps. |
The Rest of the Case
Otherwise well recently, no sick contacts, no exotic travel history.
Associated symptoms; no chest pain, syncope or palpitations, maybe some left thigh pain but only on prompting
A distant history of what sounds like an unprovoked DVT with unclear follow up but hasn't been on "the rat poison" for years.
Otherwise well recently, no sick contacts, no exotic travel history.
Associated symptoms; no chest pain, syncope or palpitations, maybe some left thigh pain but only on prompting
A distant history of what sounds like an unprovoked DVT with unclear follow up but hasn't been on "the rat poison" for years.
Clinical Examination
| Looks dreadful! Cyanotic but talking in short phrases RR 70 Sats 84% RA (89-91% 15L NRBM) BP 96/48 HR 120 Afebrile | Good AE (when she can) HSD NM JVP approx 6cm Calves SNT without pedal oedema |
So Whats Up?
Such sudden drastic deterioration is likely due to a heart (AMI), lung (PXT) or vascular problem (PE, Dissection in coronaries).
And sepsis...sepsis is always on the radar
Such sudden drastic deterioration is likely due to a heart (AMI), lung (PXT) or vascular problem (PE, Dissection in coronaries).
And sepsis...sepsis is always on the radar
Investigations
Bedside
ECG - Sinus Tachy, maybe some R heart strain but definitly nothing to catheterise at this stage
VBG - machine broken, being sent to the lab
BSL - 9
Cxr - radiographer on the way
The patients sick and the decision is made for CT to rule out the immediate life threats in the not-so-good looking patient.
CT
So what are we going to order? Non-Con vs CTPA vs Aortagram vs CTCA? The hooves sound like horses so lets go with the CTPA...
Bedside
ECG - Sinus Tachy, maybe some R heart strain but definitly nothing to catheterise at this stage
VBG - machine broken, being sent to the lab
BSL - 9
Cxr - radiographer on the way
The patients sick and the decision is made for CT to rule out the immediate life threats in the not-so-good looking patient.
CT
So what are we going to order? Non-Con vs CTPA vs Aortagram vs CTCA? The hooves sound like horses so lets go with the CTPA...
CT Findings
Occlusive thrombus in R main pulmonary artery (shown image 1)
Thrombi in L lobar pulmonary arterial branches
Evidence of R heart strain
Flattening of the interventricular septum
Reflux of contrast into the hepatic arteries and IVC (shown image 2)
Occlusive thrombus in R main pulmonary artery (shown image 1)
Thrombi in L lobar pulmonary arterial branches
Evidence of R heart strain
Flattening of the interventricular septum
Reflux of contrast into the hepatic arteries and IVC (shown image 2)
PE GRADING
American Heart Association Grading
American Heart Association Grading
| MASSIVE SBP< 90mmHg (15mins or ionotropes) OR Profound bradycardia with signs of shock OR Pulselessness (this is bad) | SUBMASSIVE SBP>90mmHg with evidence of RV dysfunction (on CTPA, Echo or "Biomarkers") | NON-MASSIVE Everything else! |
So What's Our Patient Have?
SBP > 100mmHg + CTPA shows RV dysfunction + Oh, and the bloods are back...hsTn 119 = SUBMASSIVE
SBP > 100mmHg + CTPA shows RV dysfunction + Oh, and the bloods are back...hsTn 119 = SUBMASSIVE
Right, What Do We Do?
Nothing or Anticoagulant or Lyse (systemic or interventional radiology) or Embolectomy or Nothing
Nothing or Anticoagulant or Lyse (systemic or interventional radiology) or Embolectomy or Nothing
| Some Evidence Around Lysis... | (click on pictures for articles where available) |
 Fibrinolysis for Patients with Intermediate-Risk Pulmonary Embolism (PEITHO Trial) 2014
NNT 33 vs NNH 13.7 Trend toward decreased mortality (non-sig) but increased bleeding (non-sig). Does not support thrombolysis in submassive PE |  Moderate Pulmonary Embolism Treated With Thrombolysis (from the “MOPETT” Trial) 2013
ARR 41%, NNT 2.4 Difficult to interpret study as measured echocardiographic outcomes |  Systematic review and meta-analysis for thrombolysis treatment in patients with acute submassive pulmonary embolism. 2014
|
The Internet...What Does The Internet Have To Say?
- There is a role for thrombolysis in submassive PE.
- The ‘Submassive’ group is too disparate to find an effect based on current definitions.
"Fullers Faith"
Named after the practitioner who provided most of the above information, it is a stream of consciousness that consolidates the evidence and the stuff between the lines
Named after the practitioner who provided most of the above information, it is a stream of consciousness that consolidates the evidence and the stuff between the lines
- Some "submassives" are on the way to being massive
- Thrombolysis zeal post N=1 has deflated
- Still a little confused but less than before
All This Talk About Death...What That About?
PESI (Pulmonary Embolism Severity Index) scores 30 day mortality (does not include all the following)
PESI (Pulmonary Embolism Severity Index) scores 30 day mortality (does not include all the following)
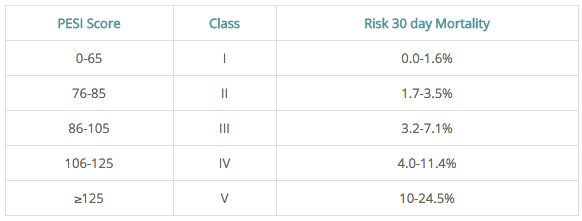 | Suggested Interpretation of Score Very Low (≤ 65) or Low Risk (66-85) by the PESI score.
|
 RSS Feed
RSS Feed