
 | Dominic Lang, David Choi, Viet Tran A 72 year old female presents to the ED following an unheralded syncopal episode. An ECG is performed. |
What does the ECG show?
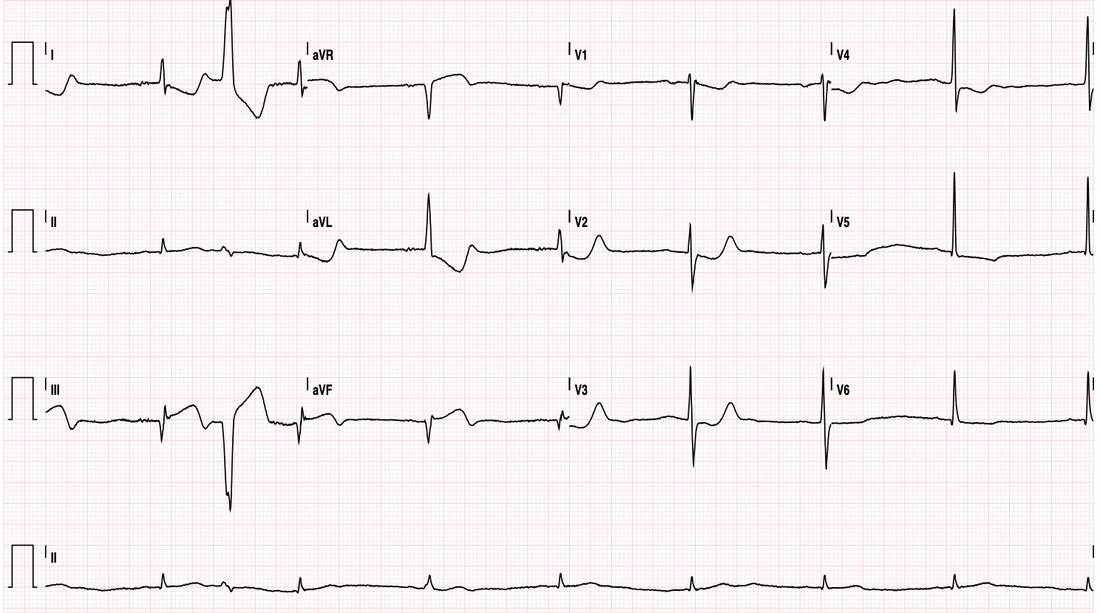
The ECG shows inferior, posterior & very likely RV STEMI as evidenced by:
- inferior: STE + Q in II III aVF, reciprocal STD I aVL
- posterior: STD + prominent R + upright Ts anteriorly (so this STD isn't reciprocal to the inferior STEMI)
- RV: STE III > II, ST isoelectric V1 with STD V2
- inferior: STE + Q in II III aVF, reciprocal STD I aVL
- posterior: STD + prominent R + upright Ts anteriorly (so this STD isn't reciprocal to the inferior STEMI)
- RV: STE III > II, ST isoelectric V1 with STD V2
How would you manage this patient?
So its a STEMI - thats straightwaord...thrombolysis (if no contraindications) and/or PCI (if available).
But what about the RV involvement?
Remember that RV involvement requires consideration of preload, as a reduction in this can be fatal.
Caution with GTN is therefore a MUST. Adequate fluid resuscitation should also be central to resuscitation,.
Given the pattern, the culprit is very likely a proximal RCA lesion.
Remember that the RCA commonly supplies the AV node (and often the SA node) and therefore conferring a high risk for arrhythmia. In retrospect - it was very much possible that the cause of the syncope was a bradyarrhythmia. My guess that's the cause of bradycardia.
This lady was appropriately resuscitated with fluid and limited GTN and transferred to the cath lab where a proximal RCA lesion was identified and stented. She is now on the road to recovery.
But what about the RV involvement?
Remember that RV involvement requires consideration of preload, as a reduction in this can be fatal.
Caution with GTN is therefore a MUST. Adequate fluid resuscitation should also be central to resuscitation,.
Given the pattern, the culprit is very likely a proximal RCA lesion.
Remember that the RCA commonly supplies the AV node (and often the SA node) and therefore conferring a high risk for arrhythmia. In retrospect - it was very much possible that the cause of the syncope was a bradyarrhythmia. My guess that's the cause of bradycardia.
This lady was appropriately resuscitated with fluid and limited GTN and transferred to the cath lab where a proximal RCA lesion was identified and stented. She is now on the road to recovery.
 RSS Feed
RSS Feed