
 | A 70 year old female interstate tourist presented to the ED to request a prescription for her blood pressure medication. She happened to mention that she has been more dyspneic over the last 2 weeks but put this down to travelling. An ECG was performed... Assume normal paper speed |
So whats wrong with the ECG?
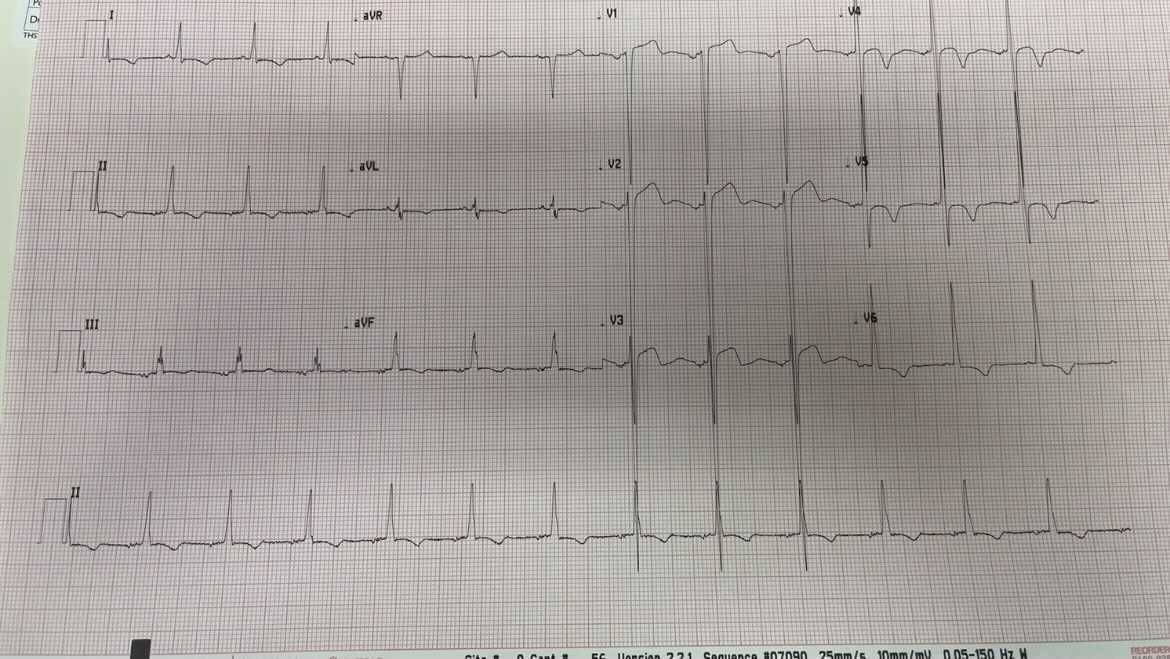
Rate: 84 BPM (Atrial) 42 BPM (Ventricular)
Normal axis
Every 2nd P-wave doesn't produce a QRS complex (in fact, non-conducting P waves are superimposed on the preceding T wave)
QRS is wide
Normal axis
Every 2nd P-wave doesn't produce a QRS complex (in fact, non-conducting P waves are superimposed on the preceding T wave)
QRS is wide
What does this mean?
A dropped beat every 2nd p-wave...so some sort of heart block...either Mobitz I or Mobitz II.
Mobitz I (aka Wenckebach) is where the PR interval increases until a P wave isnt conducted, but then resumes where it started. These are usually benign.
Mobitz II is where the PR interval is fixed, but P waves don't conduct in an (often) fixed ratio. These are not benign and need intervention (with a PPM)...and atropine often makes it worse!
So which one is this one?
A tricky (not trick) question!
It can be hard to tell with a 2:1 block (there isn't enough PR intervals to tell if they're getting longer or not)
Patient history and QRS are the main differentiators:
1. Patient History: Mobitz II is not benign, so a history of syncope is telling
2. QRS: 75% of blocks from Mobitz II are from pre-existing LBBB or bifasicular block - but the caveat to this is that 25% will have a normal QRS and that someone with Mobitz I may have a pre-existing bundle branch block!
Mobitz I (aka Wenckebach) is where the PR interval increases until a P wave isnt conducted, but then resumes where it started. These are usually benign.
Mobitz II is where the PR interval is fixed, but P waves don't conduct in an (often) fixed ratio. These are not benign and need intervention (with a PPM)...and atropine often makes it worse!
So which one is this one?
A tricky (not trick) question!
It can be hard to tell with a 2:1 block (there isn't enough PR intervals to tell if they're getting longer or not)
Patient history and QRS are the main differentiators:
1. Patient History: Mobitz II is not benign, so a history of syncope is telling
2. QRS: 75% of blocks from Mobitz II are from pre-existing LBBB or bifasicular block - but the caveat to this is that 25% will have a normal QRS and that someone with Mobitz I may have a pre-existing bundle branch block!
Where to from here?
At the very least, give her the script she came here for (if its not contraindicated).
Regarding the 2nd degree heart block - erring on the side of caution, she deserves a period of telemetry to try and capture a longer segment prior to dropping a beat (fixed ratios for Mobitz I or II often drift transiently into 3:1)
Regarding the 2nd degree heart block - erring on the side of caution, she deserves a period of telemetry to try and capture a longer segment prior to dropping a beat (fixed ratios for Mobitz I or II often drift transiently into 3:1)
 RSS Feed
RSS Feed