
 | Viet Tran Your ambulance crew have alerted you to a 59yo male who they were called to for chest pain & had a witnessed VF arrest en route that responded to an initial shock...lucky you ate breakfast. |
The nurse pulls off an ECG whilst you listen to a podcast on Targeted Temperature Management (the new 'therapeutic hypothermia' that everyone is talking about), & lets be honest, you'd get the leads the wrong way around if you tried...
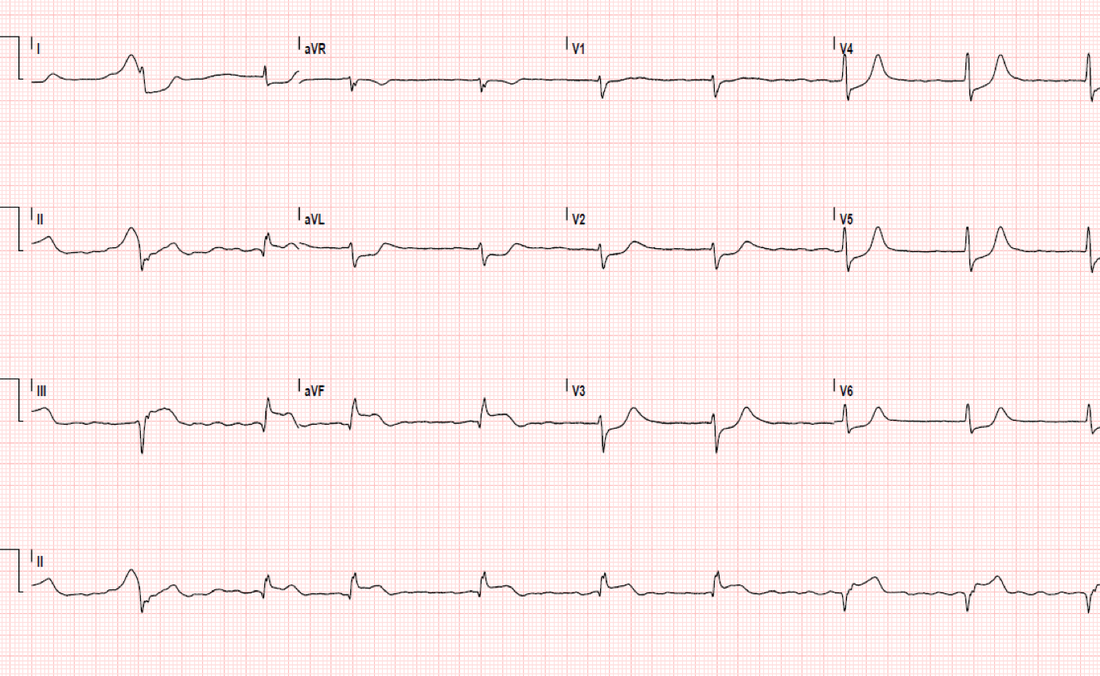
What are the significant findings?
Get this guy to a cath lab or some lytic juice...stat! He's got ST elevation in 3 concordant leads; II, III, aVF (the inferior leads, supplied by the RCA). And the reciprocal leads (I, aVL) have ST depression. V2-6 also show evidence of ST depression. Q waves are also present in lead II (the rhythm strip more so than the 12 lead), the last beat of III & aVF.
In summary - he's having an inferior STEMI - with PCI confirming a proximal RCA lesion.
Inferior STEMIs
These guys do better than the old "widow maker" anterior infarct & account for about 40% of all AMI.
They do however have nuanced characteristics to take note of:
In summary - he's having an inferior STEMI - with PCI confirming a proximal RCA lesion.
Inferior STEMIs
These guys do better than the old "widow maker" anterior infarct & account for about 40% of all AMI.
They do however have nuanced characteristics to take note of:
- 40% have concomitant right ventricular infarcts = badness when given nitrates (remember, they're dependant on preload)
- 20% will get bradycardia from 2nd or 3rd degree HB from AV node infarct
- "Some" will also extend to a posterior infarct = badness all round
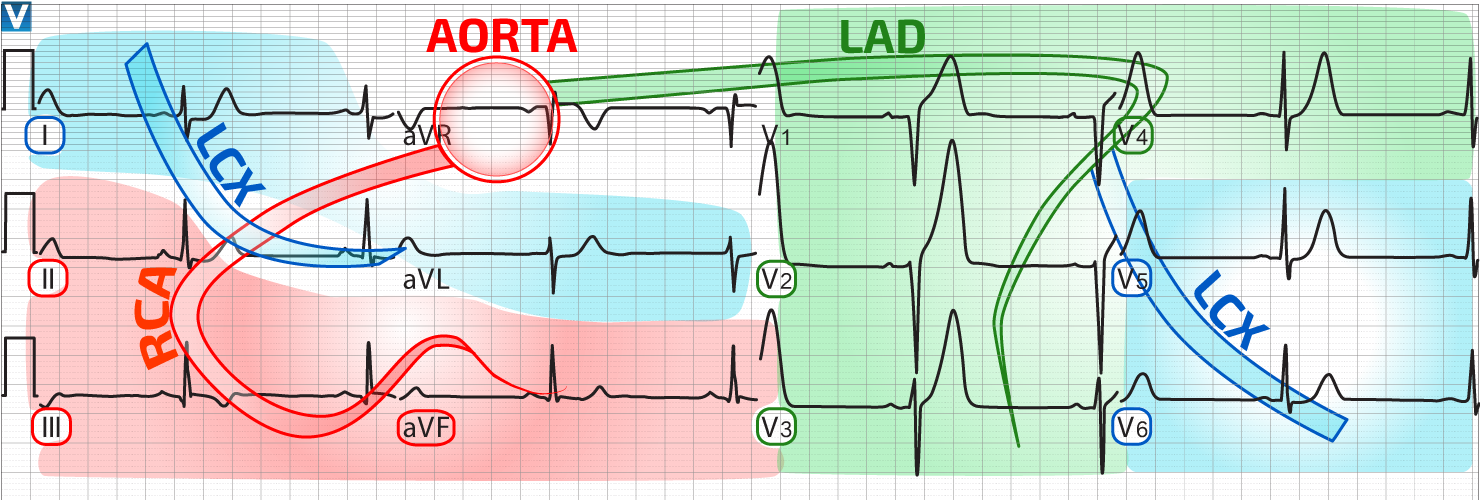
Here's a handy diagram i found thevent.org (here) to remind us of the territories each lead represents
 RSS Feed
RSS Feed