
 | Viet Tran A general overview of the different types of diving related barotrauma - read on... |
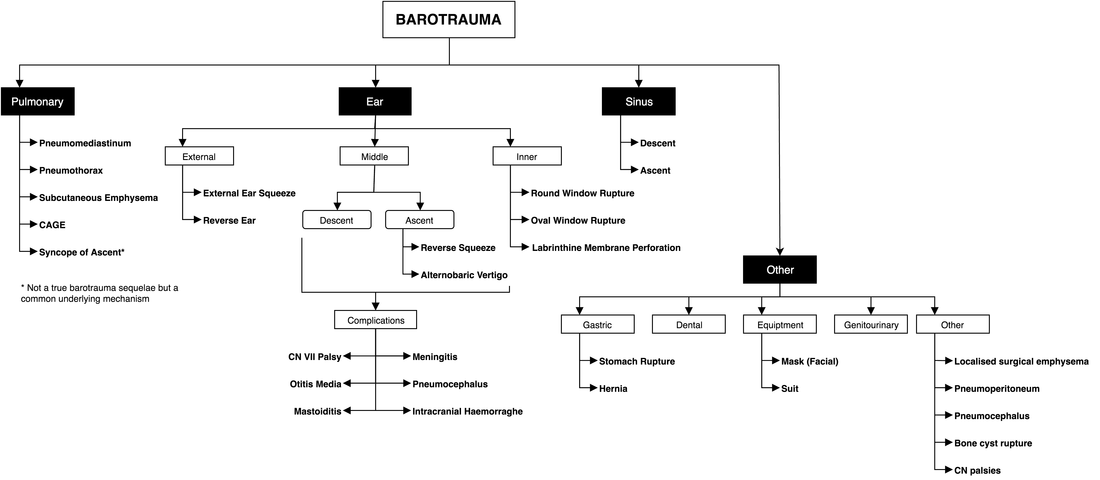
OverviewThe principles of Boyle's Law and Pascal's principle are fundamental to the mechanisms of barotraumaEarExternal
Middle
MEBtD
In the non-communicative eustachian tube, as you descend, the middle ear gas volume contracts with the end result being a vacuum effect where the TM is sucked into the middle ear, rupturing capillaries along the way and eventually decompressing either via TM perforation or the eustachian tube (whichever is least resistant)
Causes
Clinical features
MEBtA
As you ascend, the middle ear gas volume expands. If gas can't escape from the middle ear, the pressure build up can de-gas laterally through the TM or medially through the oval window (or less commonly, the round window).
Causes
Owing to the fact that most people with tube dysfunction will be caught on descent, it is less common than MEBtD. However, it is not rare, and causes can include decongestants wearing off or, if unlucky, eustachian tube dysfunction not obvious on descent.
Implications
This is problematic because of an inability to ascend
Clinical Features
MEBtS (O2 Ear)
Otoscopic Grading of MEB
Grade 0: Pain, no clinical findings
Grade 1: TM injection - notable along the handle of the malleus
Grade 2: Slight haemorrhage behind TM
Grade 3: Gross haemorraghe behind TM
Grade 4: Free blood behind TM
Grade 5: Perforation
Management of MEB
General
Grade Dependant
0-1: Diving/Flying restrictions for approx 5-7 days (usual time for resolution)
2-4: Diving/Flying restrictions for approx 6 weeks (time to blood resportion)
5: Keep ears dry, Diving/Flying restrictions for approx 6-12 weeks (time to heal), Antibiotics, surgery if no resolution (successful in 90% of patients)
Inner
Mechanism of action
Treatment
Treatment
Mask Squeeze (Facial Squeeze)
Skin Barotrauma of Descent (Suit Squeeze)
Complications
Treatment
Covered laterGastric
- Occurs during descent (or both in dry diving)
- Obstruction in the external auditory canal (EAC) causes an "air pocket" between the obstruction and the tympanic membrane (TM). On descent this air pocket can't be 'cleared' and causes a phenomenon similar to 'reverse squeeze' with the TM being sucked into the air pocket
- In dry diving, more air can enter on descent (given the rise in pressure), be trapped in this air pocket, and expand on ascent
- Causes of obstruction include: tight fitting hoods, exostoses, wax
Middle
- Includes Middle Ear Barotrauma of Descent (MEBtD), Ascent (MEBtA) and Surface (MEBtS)
- Due to eustachian tube problems - examples include dysfunction (found in 20% of population), transient narrowing/blocking (eg allergies, URTI, Samter's triad) and anatomical
MEBtD
In the non-communicative eustachian tube, as you descend, the middle ear gas volume contracts with the end result being a vacuum effect where the TM is sucked into the middle ear, rupturing capillaries along the way and eventually decompressing either via TM perforation or the eustachian tube (whichever is least resistant)
Causes
- Inexperience (most common)
- Physiological eustachian tube dysfunction (up to 20% of the population)
- Pathological eustachian tube dysfunction (eg polyps)
- Transient eustachian tube dysfunction (eg URTI, rhinitis)
Clinical features
- Pain (common)
- Hearing loss (not sensorineural - see IEBt)
- Haemorraghic Otorrhea if TM perforated
- Epistaxis or Posterior Pharyngeal blood if decompresses through tube
- Vertigo
- Otoscopic changes - see below
MEBtA
As you ascend, the middle ear gas volume expands. If gas can't escape from the middle ear, the pressure build up can de-gas laterally through the TM or medially through the oval window (or less commonly, the round window).
Causes
Owing to the fact that most people with tube dysfunction will be caught on descent, it is less common than MEBtD. However, it is not rare, and causes can include decongestants wearing off or, if unlucky, eustachian tube dysfunction not obvious on descent.
Implications
This is problematic because of an inability to ascend
Clinical Features
- Same as MEBtA with the addition of
- Alternobaric vertigo: vertigo made worse with turning to the affected side due to unequal middle ear pressures
MEBtS (O2 Ear)
- Can occur with mixed gas, or more commonly 100% O2 diving
- During the dive the middle ear fills with O2
- On the surface, if the middle ear is not equalised (and filled with air) the O2 will eventually be removed from the airspace via metabolic processes and create a vacuum
- Eventually this vacuum is strong enough to suck the TM into the middle ear causing the stages of barotrauma (much like MEBtD)
Otoscopic Grading of MEB
Grade 0: Pain, no clinical findings
Grade 1: TM injection - notable along the handle of the malleus
Grade 2: Slight haemorrhage behind TM
Grade 3: Gross haemorraghe behind TM
Grade 4: Free blood behind TM
Grade 5: Perforation
Management of MEB
General
- Prevention: frequent ear clearing BEFORE symptoms, descend in 'head-up' position, yo-yo for max 1 m (2 goes only)
- Avoid Valsalva or straining (eg lifting heavy things)
Grade Dependant
0-1: Diving/Flying restrictions for approx 5-7 days (usual time for resolution)
2-4: Diving/Flying restrictions for approx 6 weeks (time to blood resportion)
5: Keep ears dry, Diving/Flying restrictions for approx 6-12 weeks (time to heal), Antibiotics, surgery if no resolution (successful in 90% of patients)
- 'dry' perforations spontaneously heal > 90% - keep dry in meantime
Inner
- Sensorineural (or combined) hearing loss (esp high fq) + tinnitus or demonstrable vestibular damage = IEBt
- Onset can be on descent, ascent or delayed a few hours after surfacing
- Round window most often implicated, with oval window and labrynthine membrane sometimes (remember MEBt is more commonly the oval window)
Mechanism of action
- During descent, unable to equalise middle ear -> TM being sucked into the middle ear -> transmits pressure to malleolus/incus/stapes -> inward pressure on oval window -> outward pressure on round window (dalton's law) -> perforation
- Raised CSF pressure (eg valsalva) -> patent cochlear aqueduct -> round window perforation (NB aqueduct constricts with age - this is seen more often in kids)
Treatment
- Baseline audiometry & sensorineural testing (webers and Rhinne's using 512 Hz tuning fork)
- Weber's: Place in middle of forehead, if unilateral sensorineural loss, will lateralise to normal ear (vs conductive, which will lateralise to abnormal ear)
- Rhinne's: Place in front of ear then behind the air, a positive test is where air > bone = sensorineural vs bone > air = conductive
- Avoid raising CSF pressure (eg valsalva, sneezing, lifting heavy things)
- Bed rest at 30 deg head up
- Operative Mx within 24-48hrs if no improvement with conservative measures and severe (1-2 weeks if not severe)
- Counsel re: return to diving (advise against if unprovoked, no return to to baseline or ongoing tube problems)
- HBOT is questionable - remember they need to valsalva on the way down!
- A problem with descent (aka sinus squeeze) (68%) and ascent (32%)
- Maxillary sinuses most commonly implicated (usually due to polyps obstructing)
- Clinical features include pain (frontal, ethmoid, dental), epistaxis, headache
- Long term complications uncommon
Treatment
- Rest from diving until precipitating factor (eg intercurrent URTI) settles
- Corrective surgery if anatomical issue eg FESS
- Return to diving with instructions eg feet first descent, equalize ahead of depth
Mask Squeeze (Facial Squeeze)
- The mask creates a pocket of air between itself and the face
- On descent, as the air compresses, it sucks in surrounding structures - the most malleable being the face
- This is prevented by exhaling into the mask
- Its rarely serious (exception being orbital haemorraghe)
Skin Barotrauma of Descent (Suit Squeeze)
- From dry suits mostly (and sometimes poorly fitting wetsuits)
- Air stuck in suit folds compress and suck in skin with it
- Not serious, no intervention required
- From gas in dentition eg infected teeth, bone cysts, cast crowns (zinc phosphate or glass ionomer cement > resin)
- Causes pain going down as the pocket of air sucks in (usually) blood and soft tissue
- If the descent was slow these effects may go unnoticed, and with ascent pain ensues
- Occurs with ascent and is the least benign of all the barotraumas
- Due to boyles law - inspiring gas under pressure and retaining that gas with a breathe hold will expand the lungs on ascent causing alvoeli rupture
- Should be foremost thought for any uncontrolled (or unknown) ascent with problems at surface
- Unclear who is predisposed but more likely due to shearing problems eg adhesions and dynamic hyperinflation (eg asthma)
Complications
- Pneumothorax
- Arterial Gas Embolism
- Mediastinal Emphysema
- Subcutaneous Emphysema
Treatment
Covered laterGastric
- Swallowed air in stomach can cause distention on ascent -> pain, nausea, vomiting
- Uncommon causes include ingestion of carbonated drinks prior to diving
- Needless to say this is rare
 RSS Feed
RSS Feed