
 | Viet Tran Let's go over some of the 'tables' used in hyperbaric oxygen therapy (HBOT), and permutations in certain diving circumstances |
Summary
- RN62/USN6 is the standard - with variations in length depending on disease progression
- For sicker patients can consider an initial "Deep spike" to quickly compress bubbles eg USN6A or COMEX 30
- RN61/USN5 may be used for 'mild' DCS or the "worried well"
- Conservative management in the form of "Bend-watch" is also another option for the 'worried well'
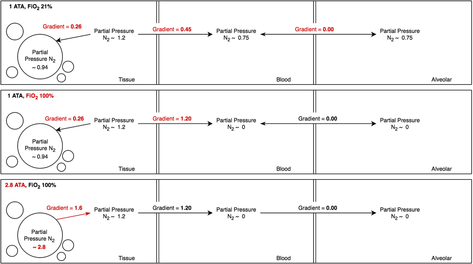
- Increases pressure gradient away from tissues and blood - see figure 1 at 1 ATA FiO2 21%, 1 ATA FiO2 100% and 2.8 ATA FiO2 100%
- Decreases bubble size and diameter to decrease mechanical effects
- Hyperoxygenate ischaemic tissue
- Decreases leukocyte adhesion and minimise the endothelial response to DCS
The Standard: RN62 (USN6)
- Royal Navy 62 (RN62 or US Navy Table 6) is the standard of care for the treatment of DCI
- The diver is in a chamber with an attendant, the chamber is filled with air
- FiO2 100% is given to the patient either via a hood or via a BIBS (built in breathing system) mask
- The chamber is compressed to 2.8 ATA (18m) and once at the bottom, FiO2 100% is applied to the diver
- Air breaks occur after 20min of FiO2 100% to minimise oxygen toxicity
- After the 3rd air break, ascent to 1.9 ATA (9m) with FiO2 100% for 60min with a 5min air break and another 60min on O2 followed by ascent (Attendant also breathing O2 on ascent to washout N2)
Variations
- You can extend the 2.8 ATA limit by 2 further 20min sessions on O2
- You can also extend the 1.9 ATA limit by a 2 further 60min sessions on O2
- Beyond these, limits, the N2 load in the attendant will require further deco stops
- If the patient becomes symptomatic on arrival at 1.9 ATA, then you can descend back to 2.8 ATA following the extensions in point 1, or continue at 1.9 ATA with O2 on and continue with or without extensions depending on the clinical picture at each air break
Why this table?
- Most widely used
- 18 metres was chosen for 2 reason:
- Its a British Royal Navy thing - 18 metres = 60 feet
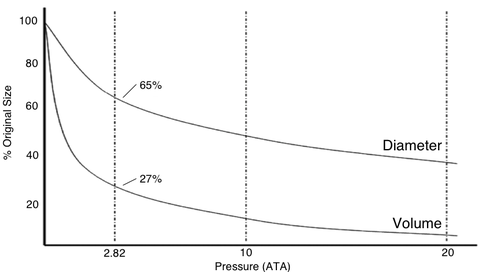
- As per figure 2 - bubble size at 2.8 ATA is 65% (diameter) & 27% (volume) of original - and past this it plateaus - ie the gain in going deeper is minimal
- By 'spiking' to a deeper depth initially, bubbles get smaller and therefore rapidly redistribute
- Ways of achieving this 'spike' include
- USN6A table (diving to 6ATA for 30min on air then ascending to 2.8 ATA as per RN62/USN6)
- Comex 30 (see below) - standard in Australia if doing a deeper dive
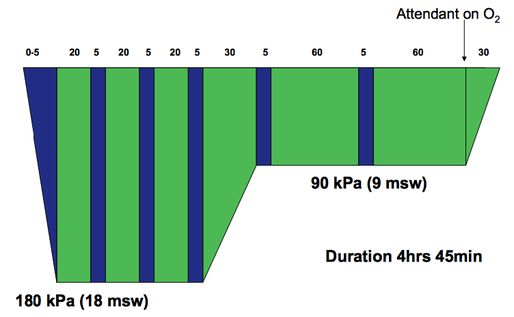
COMEX 30
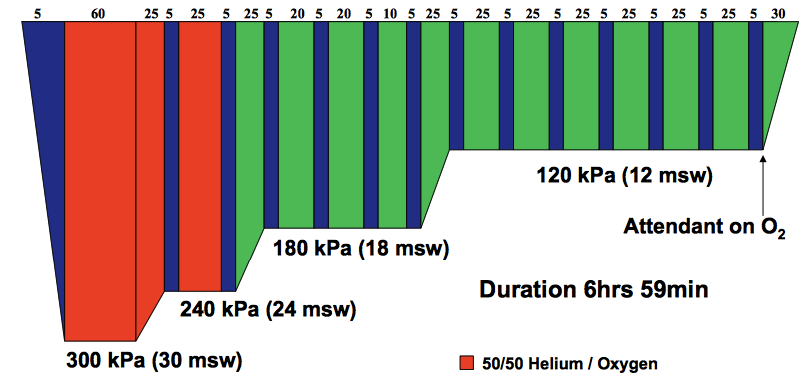
- Uncommon because many chambers are unable to accomodate for 50:50 Helium mix (necessary given the depth and subsequent risk of O2 toxicity)
- Less evidence as a result
- Previously used in Australia for neurological DCI, has fallen out of fashion given the complexities, and is now starting to come back into fashion as chambers are being updated and able to run these mixed gas tables without much difficulty
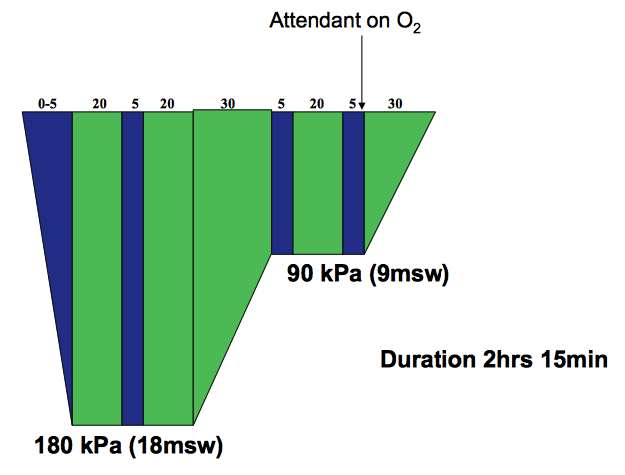
- Suggested for 'mild' or the 'worried well' (eg rapid ascent without symptoms but concerned)
- Dive to 2.8 ATA, but duration is 2 hrs 15 min
- Symptom resolution + 1 further dive or/
- Symptom plateau + 1 further dive
 RSS Feed
RSS Feed