
 | Viet Tran 61yo male OOHCA...read the rest of the story here Visiting a friend and collapsed whilst walking to the kitchen. Immediate CPR. Ambulance on scene and witnessed "good" CPR. |
So what's wrong with this ECG?
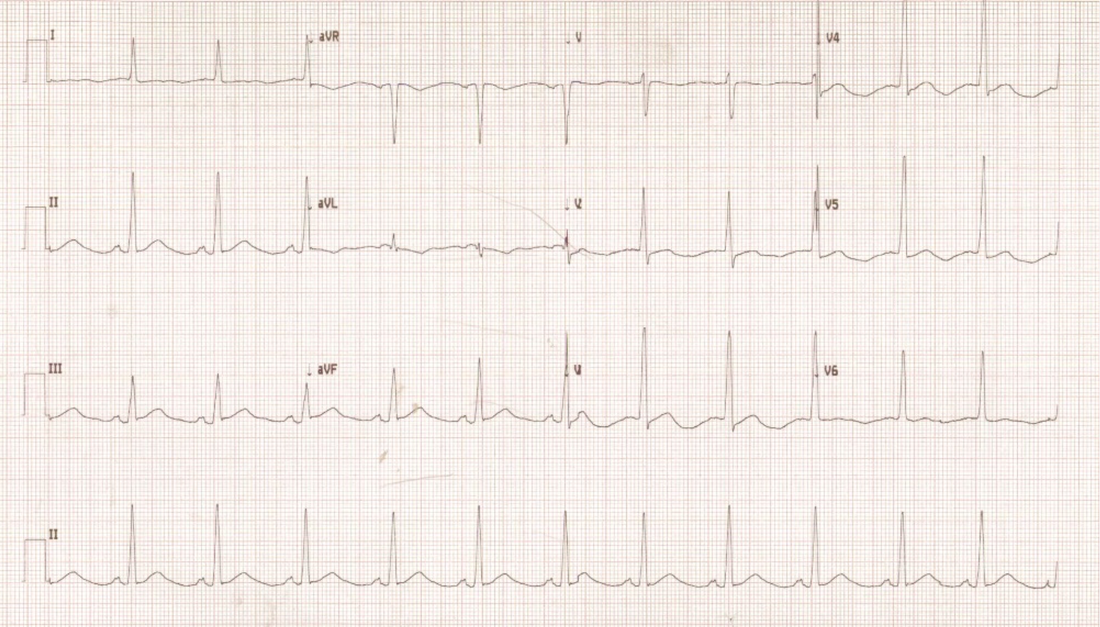
- Minor ST elevation in III, aVF
- Biphasic T-waves most marked in V2-5 and flattened in Lead I
- Associated long QT
- Suspicious for LVH
How does this fit with the patient and what's your next step?
- Non-specific findings - intracranial pathology as well as coronary thromboembolism are still on the table. See here for the discussion on OOHCA workup.
- Could also be non-specific electrolyte disturbance (identifiable on blood gas - normal in this instance) or drug ingestion if the history suggests
- A primary arrhythmia causing the OOHCA is also still a possibility
- A call to the cardiologist is definitely required
What were some of the investigation findings?
- So this man had a normal CTB & Angio
- TOE showed HCM - uneventful recovery with the requisite implanted machinary
So was there ecg evidence of HCM?
- Borderline broadened P-wave starting to become bifid in lead II (not P Mitrale yet - needs to be > 40ms between peaks). Also not diagnostic for LAE
- Borderline +ve LVH based on Sokolov-Lyon criteria (S wave depth in V1 + tallest R wave height in V5-V6 > 35 mm)
- Absence of Dagger-like Q waves in lateral > inferior leads (can be mistaken for old infarct)
 RSS Feed
RSS Feed