
 | Viet Tran Docs are increasingly feeling less reassured with the term 'stable' in medicine. Like when you say "his blood pressure is stable" because it's been 70 mmHg systolic ALL night . The same could be said with x-rays - in series, they tell a story. Here's another one... |
A 68yo female with lung cancer presented to ED with worsening SOB over the last 6 weeks, culminating in a failed effort to make it to the loo, thus precipitating today's presentation. The chest x-ray follows (click to enlarge):
 |  |
What does the x-ray show?
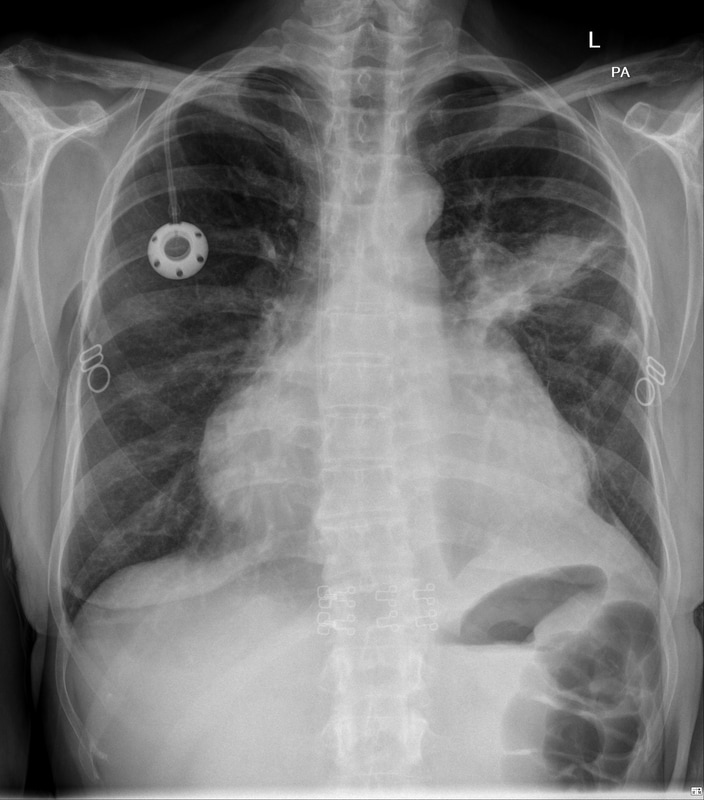
PA & lateral inspiratory film of the chest with patient identifiers missing.
Significant findings include:
1. Infus-a-port catheter inserted via the right IJV & positioned appropriately within the right atrium
2. Left peri/supra-hilar opacity in the setting of known lung cancer
3. Large cardiothoracic ratio ~ 60%
Significant findings include:
1. Infus-a-port catheter inserted via the right IJV & positioned appropriately within the right atrium
2. Left peri/supra-hilar opacity in the setting of known lung cancer
3. Large cardiothoracic ratio ~ 60%
What is your interpretation given the clinical context?
1. Without looking at the x-ray, cancer & SOB is always a concern for PE, the x-ray doesn't help to reassure us.
2. I would like to compare the left peri/supra-hilar opacity for size which may contribute to the patients SOB
3. Things like cardiac causes, anaemia etc cannot be assessed with a chest x-ray
4. The CTR is large, is this new or old?
2. I would like to compare the left peri/supra-hilar opacity for size which may contribute to the patients SOB
3. Things like cardiac causes, anaemia etc cannot be assessed with a chest x-ray
4. The CTR is large, is this new or old?
Here's a an x-ray done 1 months prior (click to enlarge):
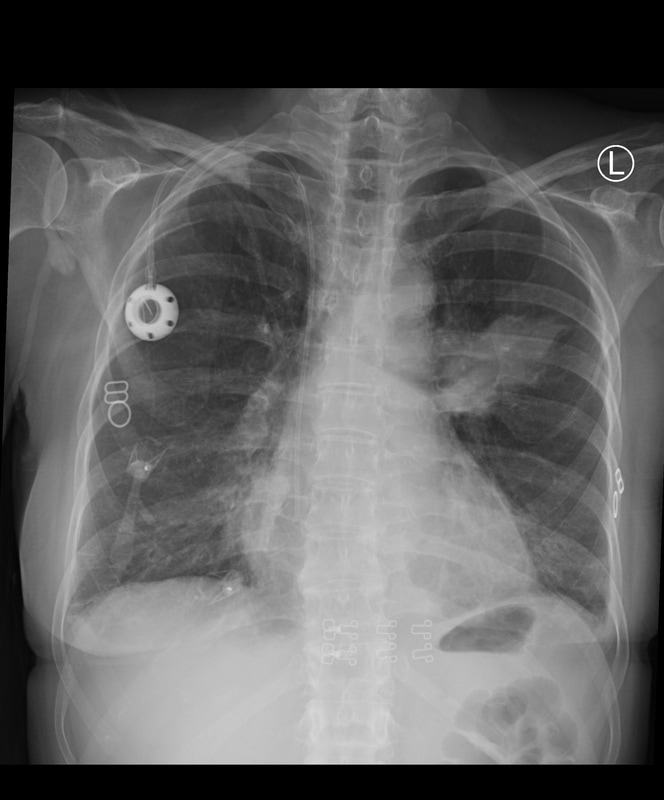 | 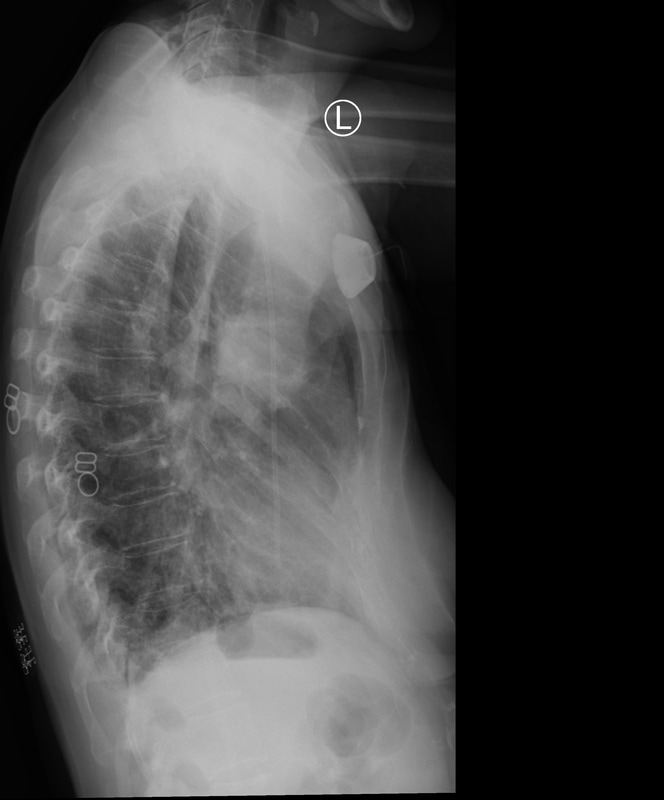 |
Has this narrowed your differential?
1. The left peri/suprahilar mass hasn't changed much in size - reduced if anything
2. The CTR however has changed over the 1 month interval (50% to 60%)
Differential diagnosis for an acutely widened CTR include
1. Expiratory film
2. Acute pericardial effusion
Clinical Correlation for tamponade physiology is pertinent
Tamponade Physiology aka Beck's Triad
For the record, non-acute widened CTR include
1. Cardiomegaly: Left ventricle, right ventricle or both
2. Cardiac tumour
3. Large epicardial fat pad (rare)
4. Chronic pericardial effusion
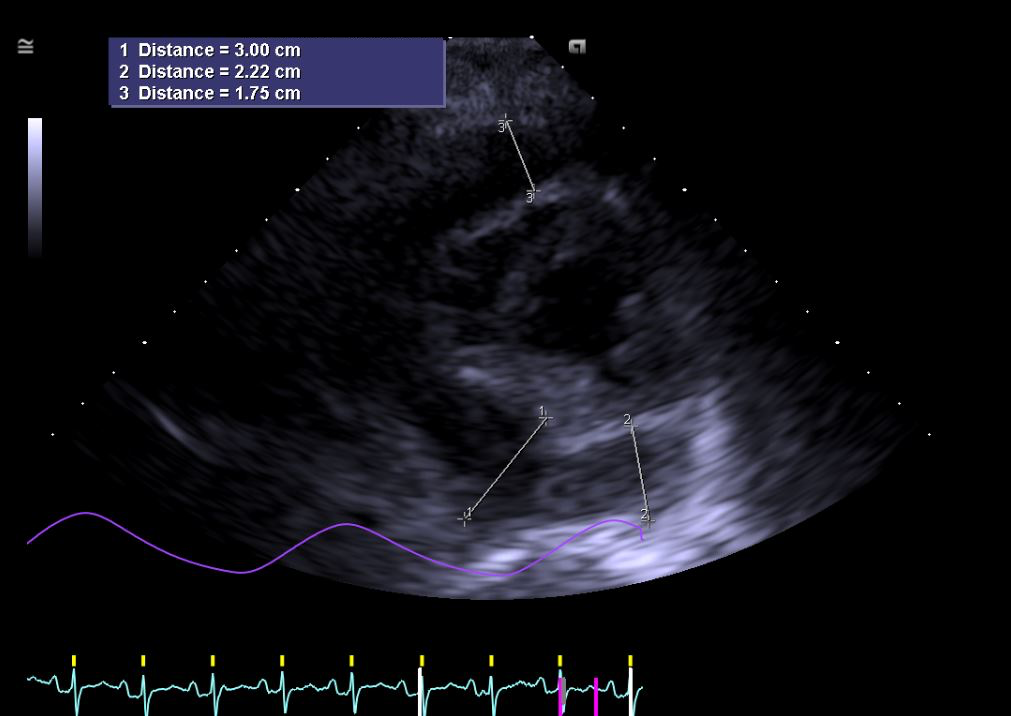
The patient went on to have an echo confirming the moderate sized pericardial effusion with 'echo' evidence of tamponade. There were no clinically obvious signs of tamponade.
2. The CTR however has changed over the 1 month interval (50% to 60%)
Differential diagnosis for an acutely widened CTR include
1. Expiratory film
2. Acute pericardial effusion
Clinical Correlation for tamponade physiology is pertinent
Tamponade Physiology aka Beck's Triad
- Low BP
- Jugulovenous distension
- Muffled Heart Sounds
For the record, non-acute widened CTR include
1. Cardiomegaly: Left ventricle, right ventricle or both
2. Cardiac tumour
3. Large epicardial fat pad (rare)
4. Chronic pericardial effusion
The patient went on to have an echo confirming the moderate sized pericardial effusion with 'echo' evidence of tamponade. There were no clinically obvious signs of tamponade.
 RSS Feed
RSS Feed