
 | David Bertoni The academic/functional territories of the brain are an important foundation - this knowledge consumed in medical school doesn’t translate precisely into discrete territory deficits that we see come through the turnstiles. This is because these functional areas do not have discrete vessel-for-territory vascular supply. Nevertheless, they do form distinct patterns of deficit when compromised - or "Stroke Syndromes". Here is a simple systematic way of differentiating supply issues for these neurons. |
Objectives
- Review basic & relevant neuroanatomy
- Describe an approach to stroke localisation based on clinical findings (ant vs post)
FRONTAL // Personality changes, anosmia, gait apraxia, leg weakness,urinary incontinence, expressive dysphasia
PARIETAL // Dysphasia, Gerstmann's syndrome (dominant) / Sensory inattention, dressing / constructional apraxia (non-localising)
TEMPORAL // Memory loss, receptive dysphasia (dominant)
OCCIPITAL // Homonymous hemianopia (contralateral)
Some Stats (unreferenced)
- Approx 80% ischaemic, 20% haemorrhagic
- Approx 80% anterior circulation, 20% vertebrobasilar
- In young and middle aged, approx 20% of non-haemorrhagic strokes are caused by cervical artery dissection
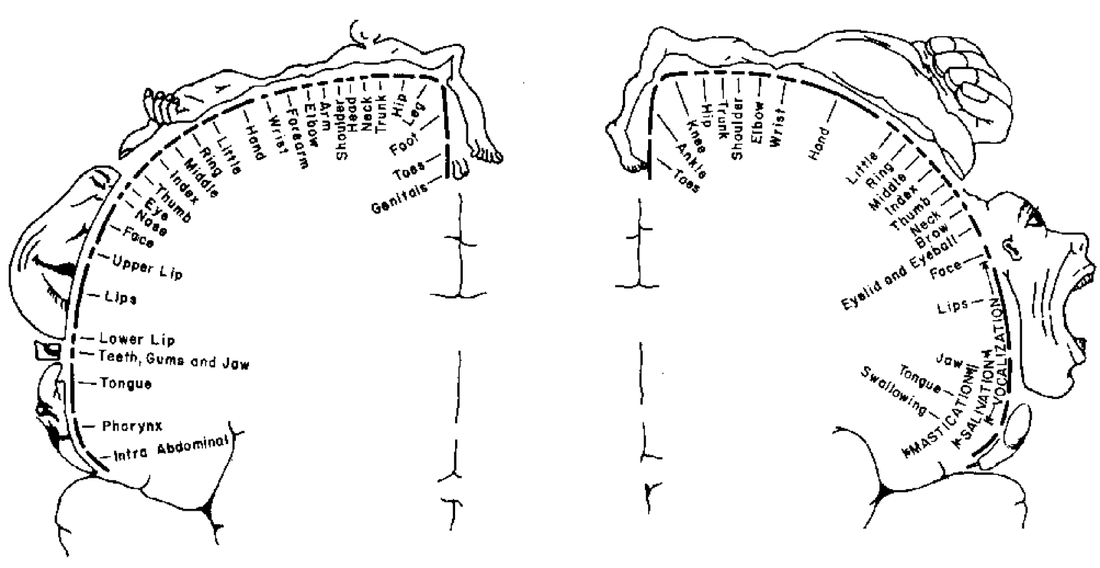
Functional Anatomy
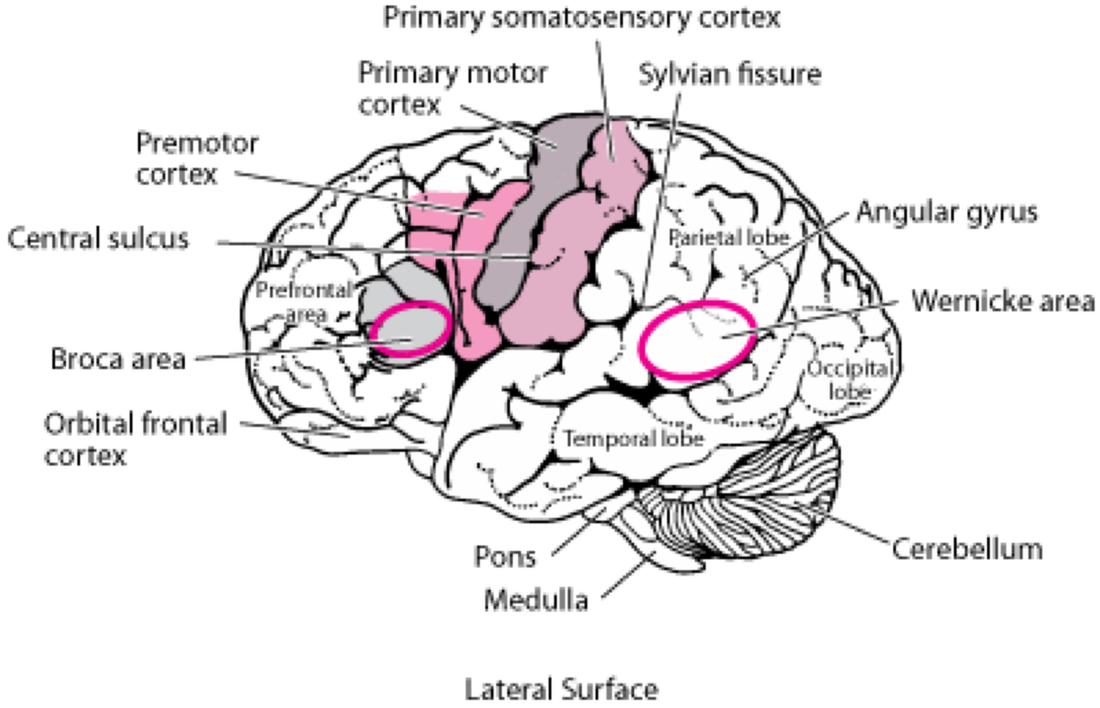 |  |
Tip: Broca's area is closest to motor cortex, therefore is the motor part of speech | Gerstmann's Syndrome |
Vascular Supply to the Brain
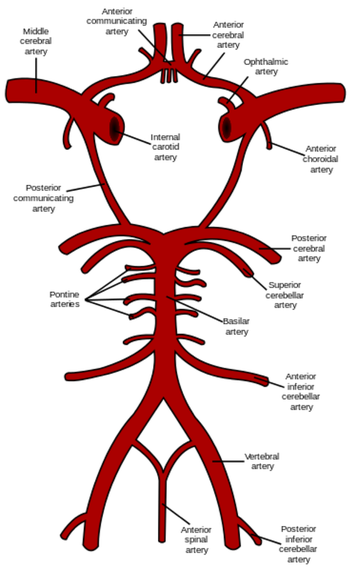 | In general, the most difficult & important aspect of understanding the vascular supply to the brain is to appreciate that it has an
Features of Posterior Circulation Strokes |
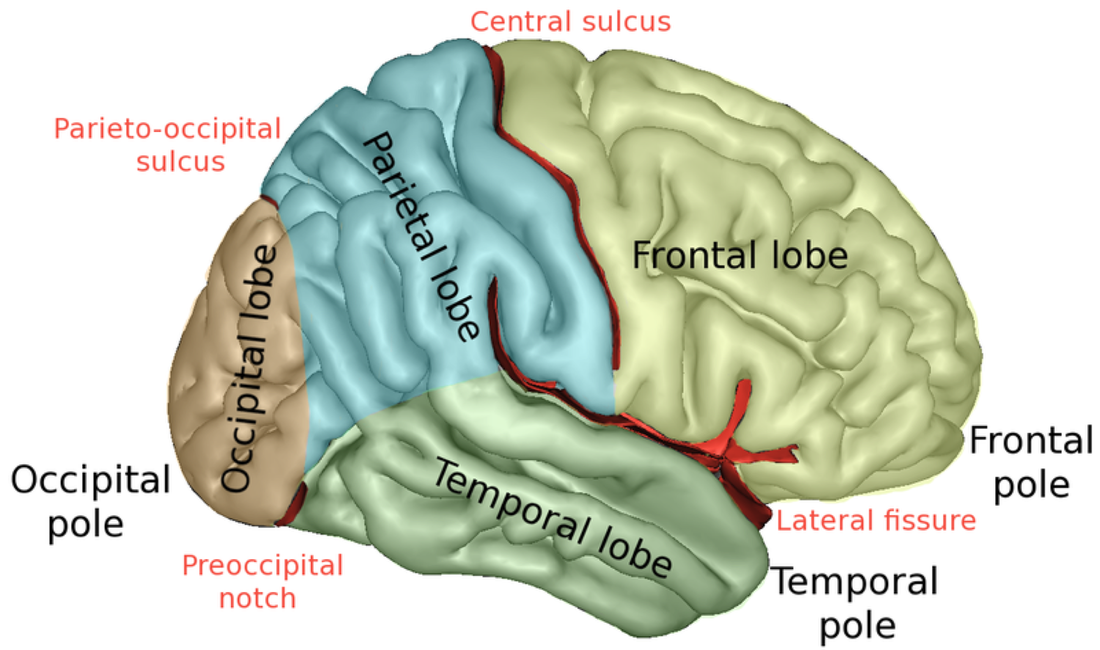
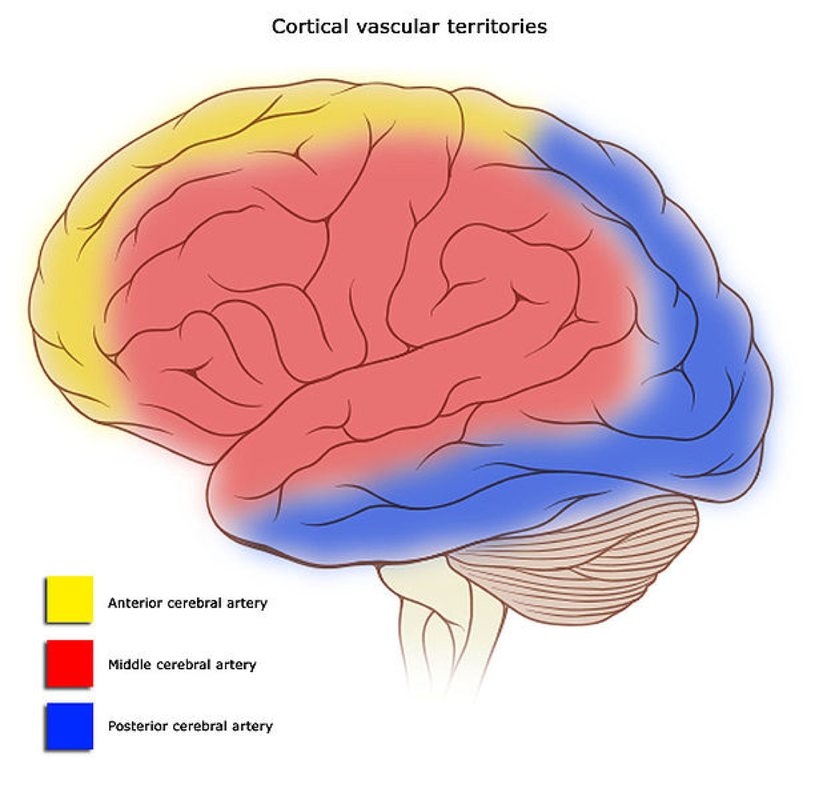
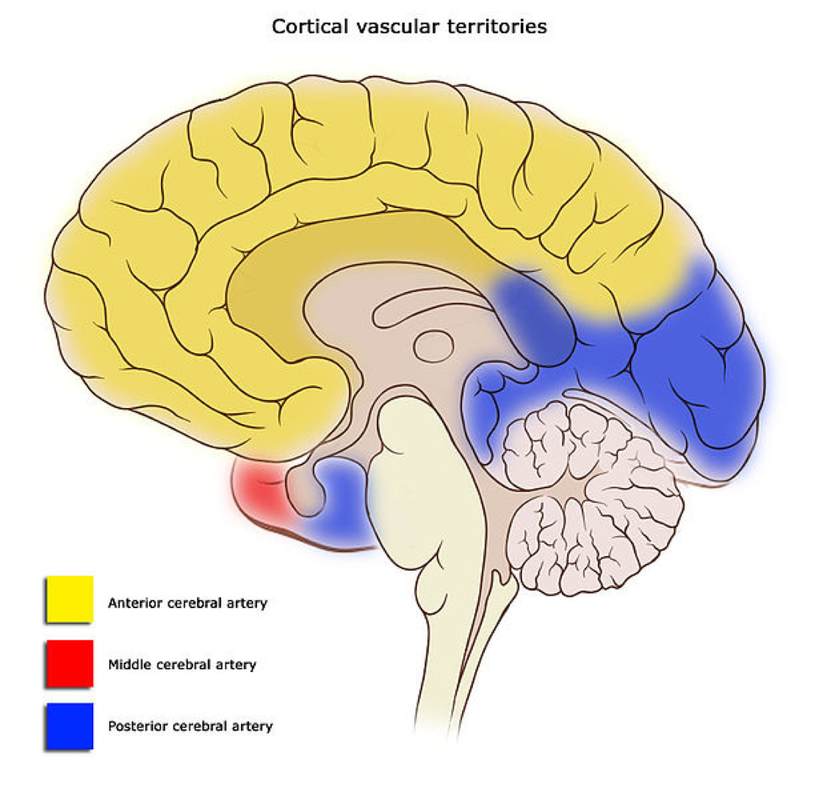
Vascular 'Territories'
| As you can see from the diagrams (right), laterally much of the supply is from the MCA (red) and medially is the ACA (yellow). If you match the vascular territory with the homunculus you can appreciate what deficits you might find based on the deficient vessel. ACA UMN leg > arm, sensory loss leg, urinary incontinence (variable) MCA UMN + sensory loss face, arm > leg, homonymous hemianopia, dysphasia (dominant), neglect (non-dominant) PCA Heminanaesthesia (thalamus), homonymous hemianopia, alexia, visual hallucination Lacunar Pure motor / sensory / sensorimotor hemiparesis (no cortical signs), ataxic hemiparesis, dysarthria – clumsy hand syndrome. |
 |
Brainstem Strokes (aka Posterior Circulation Strokes)
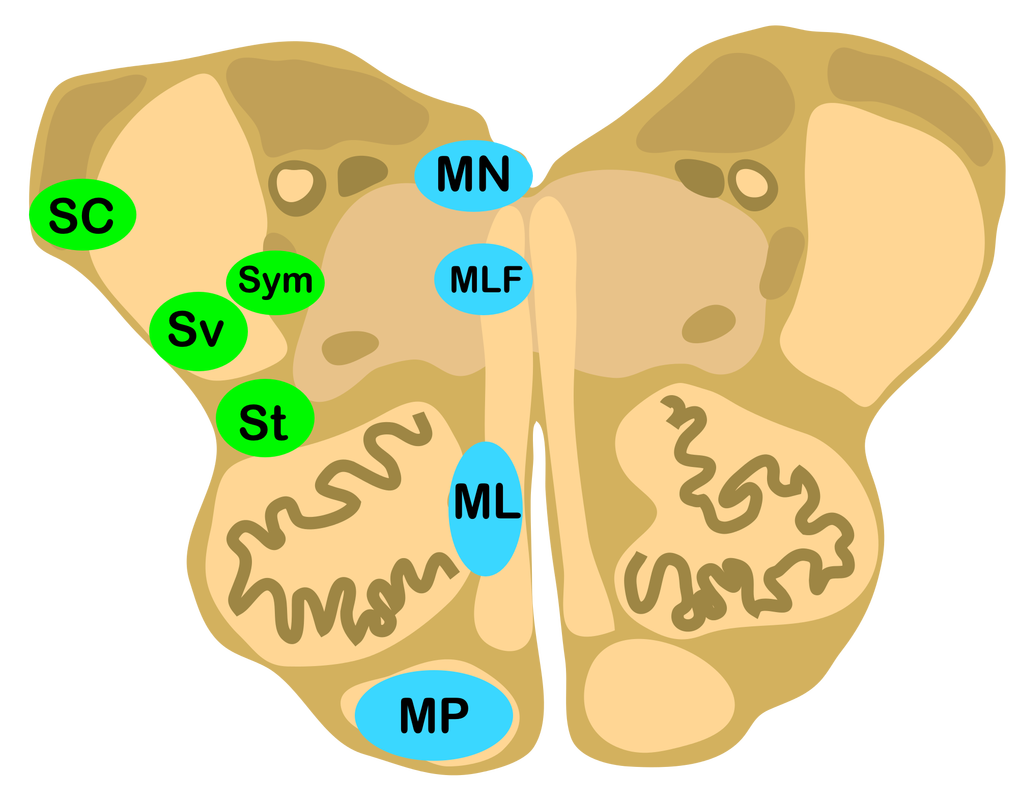 | Peter Gate's developed a "Rule of 4s for the brainstem" to simplify stroke syndromes:
NB Above rules used as meridians of longitude / latitude Video here Article here |
| LATERAL SC (Spinocerebellar)
*Partial Ptosis, Meosis & Anhidrosis | MEDIAL MN (Motor Nucleus 3, 4, 6 or 12)
**absent ipsilateral eye adduction and contralateral abducted nystagmus |
Test Cases To Determine Territory Deficit
CASE 1
| Weakness of left upper / lower limbs with facial sparing, loss of vibration & proprioception left upper / lower limbs. Tongue deviation to right. |
Conclusion: Right Medial Medullary Ischaemia |
CASE 2
| Right limb ataxia, right sided facial numbness, right facial weakness |
Conclusion: Right Lateral Pontine Ischaemia |
CASE 3
| Left limb ataxia, abnormal left pain / temperature perception in face, left Horner's syndrome, left absent gag and palate elevation. |
Conclusion: Left Lateral Medullary Syndrome |
References
- Caplan LR (2015). Posterior circulation cerebrovascular syndromes. www.uptodate.com
- Filho JO (2015). Initial assessment and management of acute stroke. www.uptodate.com
- Filho, JO (2015). Lacunar infarcts. www.uptodate.com
- Gates, P. The rule of 4 of the brainstem: a simplified method for understanding brainstem anatomy and brainstem vascular syndromes for the non-neurologist. Internal Medicine Journal 2005; 35: 263-266.
- Nickson, C. (2009) http://lifeinthefastlane.com/brainstem-rules-of-4/
- Nickson, C. (2009) http://lifeinthefastlane.com/using-the-brainstem-1/
- Tintinalli, JE editor in chief. Tintinalli's emergency medicine. A comprehensive study guide. 7th ed. [e-book]. McGraw-Hill; 2011 [cited 2015, Sep 12].
- Talley NJ, O'Connor S. Clinical examination. A systematic guide to physical diagnosis. 6th ed. Sydney; Elsevier: 2010.
 RSS Feed
RSS Feed