
 | Viet Tran Your next patients are a couple of novice marathon runners with hearts of gold. They've made thirsty work of their running attempt & have come to you for help with fatigue, vomiting & nausea... |
Gaz, A 31yo male hipster has raised a gofundme campaign to run in the half marathon. The last time he ran was in the grade 10 cross country. As such he has started training for the event this week. He presents to ED feeling fatigued, with nausea and vomiting after running (mostly walking) 5 km. He tells you that as per google he has kept up with his hydration to cover those insensible losses..and then some.
As part of his work up, he has a venous gas;
As part of his work up, he has a venous gas;
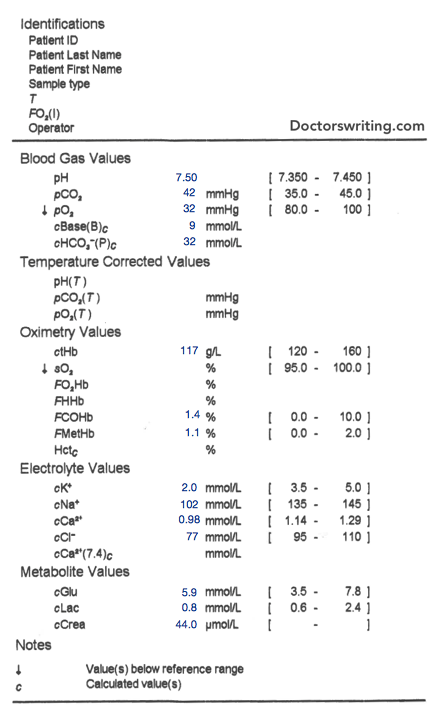
What is your interpretation?
It looks like a metabolic alkalosis with life threats that need addressing including:
He has a severe hyponatraemia (mild/mod = 120-135 mmol/L, severe = < 120 mmol/L)
- A severe hyponatraemia
- A moderately low K (2.0 mmol/L)
- A mildly low chloride
- A mildly low Ca
He has a severe hyponatraemia (mild/mod = 120-135 mmol/L, severe = < 120 mmol/L)
What is your approach to management?
If this was mild/moderate (120-135 mmol/L), you would fluid restrict from 500ml - 1L per 24 hrs (or 500ml less than daily urine output)
But this is severe. After establishing ABCD we move on to E - electrolytes. We need to replace this in the form of 3% Normal Saline (which contains 513 mmol of Na+).
WARNING: OSMOTIC DEMYLINATION is bad & irreversible. It happens when you replace Na too quickly
How quickly is too quickly?
Aim for <10 mmol in the first 24hrs & < 18 mmol in the first 48 hours. To buffer this, I suggest you aim for 6-8 mmol/day. 6 mmol if they have risk factors for osmotic demyelination (Na < 105, Low K, Chronic alcohol abuse, severe malnutrition, advanced liver disease or chronic hyponatraemia).
OK, so lets assume he's 85kg and I'm going to give 8mmol of Na over 24hrs. Now there's 513 mmol in 1L of 3% Saline...so how many ml/hr is that?
Here's the formula to work out how much a 1L bag of 3%NS will increase the [Na+]:
But this is severe. After establishing ABCD we move on to E - electrolytes. We need to replace this in the form of 3% Normal Saline (which contains 513 mmol of Na+).
WARNING: OSMOTIC DEMYLINATION is bad & irreversible. It happens when you replace Na too quickly
How quickly is too quickly?
Aim for <10 mmol in the first 24hrs & < 18 mmol in the first 48 hours. To buffer this, I suggest you aim for 6-8 mmol/day. 6 mmol if they have risk factors for osmotic demyelination (Na < 105, Low K, Chronic alcohol abuse, severe malnutrition, advanced liver disease or chronic hyponatraemia).
OK, so lets assume he's 85kg and I'm going to give 8mmol of Na over 24hrs. Now there's 513 mmol in 1L of 3% Saline...so how many ml/hr is that?
Here's the formula to work out how much a 1L bag of 3%NS will increase the [Na+]:

TBW calculations
- Female: not elderly = BW x 0.5, elderly = BW x 0.45
- Male: not elderly = BW x 0.6, elderly = BW x 0.5
So let's do the calculation:
Increase in serum [Na] = (513 - 102) / (85 x 0.6 + 1) = 411/52 = 7.9
Therefore a 1L bag of 3% N/Saline will increase the serum Na by 7.9 mmol/l. Perfect! Since we only want to increase the serum Na by 8mmol in 24hrs, we'll give the 1L bag of 3% N/Saline over 24hrs i.e. 42ml/hr
The fluids are running, he's starting to feel better & you carry on with your work. The next patient that rolls up in the back of an ambulance is his hipster mate Banjo...in fact it was his idea to maintain supra hydration post meander.
Banjo undergoes a similar workup...and as if by fate, has the same Na...and weight. So he embarks on the same management. Unfortunately for Banjo, he has a seizure in front of you...
Banjo undergoes a similar workup...and as if by fate, has the same Na...and weight. So he embarks on the same management. Unfortunately for Banjo, he has a seizure in front of you...
What do you do now?
Great! a seizure. something where calculations are not required!
ABCD. Abort the seizure.
Unlike other causes of seizure, a hyponaetremic seizure responds poorly to Benzodiazepines.
Instead, you need to get that Na up!
Give NaCl 3% 100ml over 10minutes and repeat as needed (maximum 3 times)
"But you just said that correcting too quickly causes an irreversible osmotic demyelinating pathology?!"
And right you are. It's a risk v benefit thing with the acute issue of seizure or coma reflecting the fact that this patient might be herniating, swelling or has an element of cerebral ischaemia.
So when else might you consider more rapid initial correction (not necessarily as fast as a seizure/coma)?
ABCD. Abort the seizure.
Unlike other causes of seizure, a hyponaetremic seizure responds poorly to Benzodiazepines.
Instead, you need to get that Na up!
Give NaCl 3% 100ml over 10minutes and repeat as needed (maximum 3 times)
"But you just said that correcting too quickly causes an irreversible osmotic demyelinating pathology?!"
And right you are. It's a risk v benefit thing with the acute issue of seizure or coma reflecting the fact that this patient might be herniating, swelling or has an element of cerebral ischaemia.
So when else might you consider more rapid initial correction (not necessarily as fast as a seizure/coma)?
- Intracranial pathology or increased intracranial pressure
- Known hyponatraemia for < 24-48 hrs
- Self-induced water intoxication
- Coma
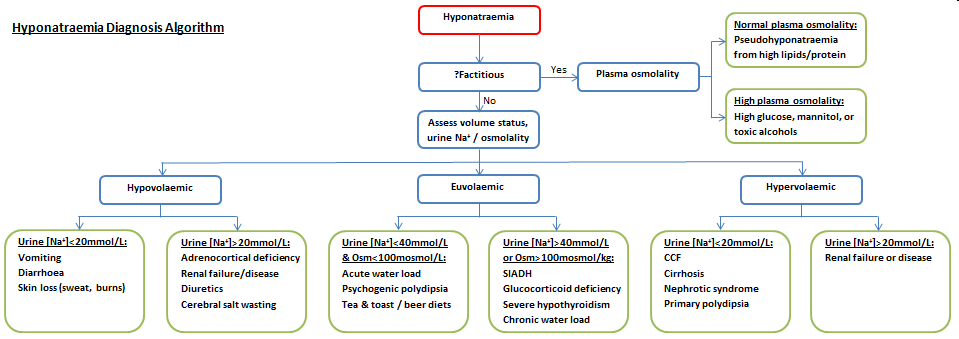
Any discussion of hyponatraemia is not complete without the good old "causes" flow chart that splits it up between hypo, eu and hypervolemic hyponatraemia.
 RSS Feed
RSS Feed