
 | Viet Tran Atrial Fibrillation (AF) is the most common cardiac arrhythmia. It makes sense that we understand how the beast works, and how we can soothe her savage soul, and work out what any of this has to do with tattoos... This is my summary of Brian Doyle's departmental talk on the subject (as well as the 2014 AHA et al guidelines for AF) |
Summary
- AF is common (20% in ages >85)
- AF with instability = electrical cardioversion
- Initial mx of AF includes identifying precipitant (PIRATES) and giving MgSO4 & K replacement (to make the doctor feel better)
- Rate vs Rhythm control: its a spectrum - healthier/younger = closer to rhythm control (within 48hrs), sicker/older = rate control
- Rate: beta blockers or calcium channel blockers are an effective first line treatment for rate control if not contraindicated, aim for HR < 110 PBM
- Amiodarone is often the first choice in critically ill patients who do not need cardioversion
- Doing "nothing" often works (as good as drugs when cardioverting - 70%, and inferior to electrical - 90%)
- Don't forget to anticoagulate according to scoring systems - drug of choice is yet to yield a clear winner for the patient
Definition
AF can be considered as rapid & disorganised electrical signals that causes the atria to contract fast and irregularly (ie fibrillate) - see the video for an example of what it looks like.
Mechanism
Think of it as atrial electrical activity initiated at ectopic foci with a funky circus rhythm, only not a circus, but a vortex. Its complicated. Its called the Rotor and Spiral Wave Model. It also applies to the ventricle. Particularly in the young, such ectopic foci are often found on pulmonary veins and amendable to ablative therapy.
Epidemiology
- Most common arrhythmia
- Uncommon in young, peaks at ~ 20% in > 85 yo
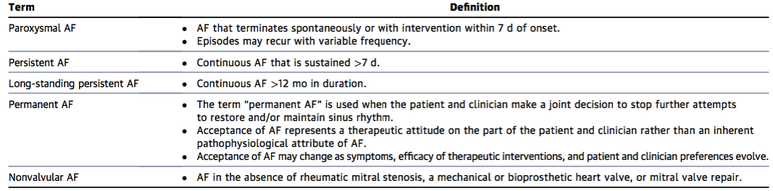
Definitions of AF
There are 5 definitions (not types) of AF for the purpose of evidence based medicine (see table below from the 2014 AHA et al guidelines on AF).
By far the most important distinguishing features are:
Valvular AF (VAF) vs Non-Valvular (NVAF)
VAF refers to patients with mitral stenosis or artificial heart valves (and valve repair in North American guidelines only - the below table was made in the USA). This distinction is important because they lead to an increase risk of stroke (that's right MR, AS, AR do not increase your risk of stroke) (1). In fact, VAF has a stroke incidence of up to 18%. More recently NVAF has been recognised as having its own stroke risk and therefore a need to anticoagulate a proportion of this population (2-10% per 100 patient years). The distinction remains because current evidence (and lack thereof) has yet to recognise the efficacy of NOACs on VAF (2).
I guess the question that i have is, given that we don't often do echos in the emergency department, and murmurs are difficult to interpret at the best of times, are we doing a disservice by discharging the unclassified AF patient with a NOAC?
Chronicity
There's a saying going around;
"AF begets AF" - or more aptly put
"What's the difference between a Tattoo and AF? You can get rid of a Tattoo"
Essentially what this alludes to is the self perpetuation of AF structurally & physiologically through tachycardia-mediated cardiomyopathy. Don't believe me? They've induced AF in goats and studied their hearts to come to this conclusion (3).
1. Fauchier, Laurent et al. "How To Define Valvular Atrial Fibrillation?". Archives of Cardiovascular Diseases 108.10 (2015): 530-539. Web.
2. Kannel, William B. et al. "Epidemiologic Features Of Chronic Atrial Fibrillation". New England Journal of Medicine 306.17 (1982): 1018-1022.
3. Finet, J. Emanuel, David S. Rosenbaum, and J. Kevin Donahue. "Information Learned From Animal Models Of Atrial Fibrillation". Cardiology Clinics 27.1 (2009): 45-54.
By far the most important distinguishing features are:
- Valvular vs Non-valvular
- Chronicity: Paroxysmal vs Persistent vs Long-standing vs Permanent
Valvular AF (VAF) vs Non-Valvular (NVAF)
VAF refers to patients with mitral stenosis or artificial heart valves (and valve repair in North American guidelines only - the below table was made in the USA). This distinction is important because they lead to an increase risk of stroke (that's right MR, AS, AR do not increase your risk of stroke) (1). In fact, VAF has a stroke incidence of up to 18%. More recently NVAF has been recognised as having its own stroke risk and therefore a need to anticoagulate a proportion of this population (2-10% per 100 patient years). The distinction remains because current evidence (and lack thereof) has yet to recognise the efficacy of NOACs on VAF (2).
I guess the question that i have is, given that we don't often do echos in the emergency department, and murmurs are difficult to interpret at the best of times, are we doing a disservice by discharging the unclassified AF patient with a NOAC?
Chronicity
There's a saying going around;
"AF begets AF" - or more aptly put
"What's the difference between a Tattoo and AF? You can get rid of a Tattoo"
Essentially what this alludes to is the self perpetuation of AF structurally & physiologically through tachycardia-mediated cardiomyopathy. Don't believe me? They've induced AF in goats and studied their hearts to come to this conclusion (3).
1. Fauchier, Laurent et al. "How To Define Valvular Atrial Fibrillation?". Archives of Cardiovascular Diseases 108.10 (2015): 530-539. Web.
2. Kannel, William B. et al. "Epidemiologic Features Of Chronic Atrial Fibrillation". New England Journal of Medicine 306.17 (1982): 1018-1022.
3. Finet, J. Emanuel, David S. Rosenbaum, and J. Kevin Donahue. "Information Learned From Animal Models Of Atrial Fibrillation". Cardiology Clinics 27.1 (2009): 45-54.
Consequences
| The clinical consequences of AF (the loss of co-ordinated atrial contraction) are manifested by 3 physiological changes (stay with me here, it makes sense): 1. Rapid Ventricular Response (RVR) RVR causes 2 things: a) Short Term: Tachycardia + short diastolic filling time = ↓ cardiac output +/- haemodynamic compromise b) Long Term: Tachycardia-mediated cardiomyopathy 2. Decreased Diastolic Filling The lack of co-ordinated contraction in itself also ↓ diastolic filling and confounds the issues of RVR & ↓ filling time to cause ↓ CO +/- haemodynamic compromise 3. Blood stasis AF sets up an environment that predisposes to intra cardiac thrombus which can lead to stroke. Clots most often form in the atrial appendage (the red bit in the picture) - which is notoriously difficult to see with a transthoracic approach to echocardiography. This is annoying, because despite the advent of point of care ultrasound, the ability to cardiovert in the stable-unknown-onset-AF patient remains elusive. |  |
Causes
This is important when we start to look at the management of AF. A familiar acronym used is "PIRATES". As with all acronyms, everything wont be covered and clinical correlation is suggested;
P Pulmonary (PE, COPD) and Pericarditis
I Idiopathic, Iatrogenic, Infarction, Infection
R Rheumatic (ie VAF), Regurgitation (mitral), Recurrence of AF
A Alcohol*, anaemia
T Thyrotoxicosis, Toxins
E Electrolytes, Endocarditis, Ectopic Foci
S Sepsis, Stimulants, Structural
*The "Holiday Heart Syndrome" refers to AF in otherwise healthy patients, triggered on the first day back at work from a bender. The suggested mechanism involving withdrawal.
P Pulmonary (PE, COPD) and Pericarditis
I Idiopathic, Iatrogenic, Infarction, Infection
R Rheumatic (ie VAF), Regurgitation (mitral), Recurrence of AF
A Alcohol*, anaemia
T Thyrotoxicosis, Toxins
E Electrolytes, Endocarditis, Ectopic Foci
S Sepsis, Stimulants, Structural
*The "Holiday Heart Syndrome" refers to AF in otherwise healthy patients, triggered on the first day back at work from a bender. The suggested mechanism involving withdrawal.
MANAGEMENT
As always, the initial management involves a combination of "ABC"
If haemodynamic instability exists - electricity is the first line management (in conjunction with appropriate sedation)
Once stability has been established there are 3 areas to address with management and 2 considerations for the patients future
+/- Maintenance of Sinus Rhythm
+/- Intervention
If haemodynamic instability exists - electricity is the first line management (in conjunction with appropriate sedation)
Once stability has been established there are 3 areas to address with management and 2 considerations for the patients future
- Precipitant
- Rate vs Rhythm vs Nothing
- Anticoagulation
+/- Maintenance of Sinus Rhythm
+/- Intervention
1. Precipitant
In some ways, AF is like constipation - it hides an underlying aetiology. Remember PIRATES? In the ED setting a suggested work up might include;
- History of PIRATES
- Bloods; looking at Hb (A), Electrolytes (E), TFTs (T)
- Outpatient Echo (R)
- MgSO4 & K replacement can be considered, no evidence exists for or against this parallel approach to managment
2. Rate v Rhythm v Nothing
For decades physicians have feuded over the management of AF. Here is a summary of the landmark studies (click on papers to get pubmed ref):
 AFFIRM 2002, RCT, n=4060 Rate v Rhythm (electricity or drugs) Primary Outcome: Mortality NO statistical difference to outcome |  RACE 2002, RCT, n=520 Rate vs Electricity only Primary Outcome: Quality of Life NO statisticl difference to outcome |  PIAF 2000, RCT, n=252 Rate v Rhythm (diltazam or amiodarone) Primary Outcome: Symptomatic Relief No statisticl difference to outcome |  STAF 2003, RCT, n=200 Rate vs Electricity only Primary Outcome: Mortality (among other things) No statisticl difference to outcome |  HOTCAFE 2004, RCT, n=205 Rate vs Electricity Primary Outcome: Mortality No statistical difference |
A few key issues and points arise from these studies
- Inclusion/Exclusion criteria were VERY heterogenous (eg AFFIRM included only those over the age of 65 years)
- Types of both rate and rhythm were heterogenous between studies
- Primary outcomes were heterogenous
- All the studies showed no difference for their primary outcomes
Rate Control
Before we jump into pharmacological heaven, we should talk about targets. HR targets given that we're trying to rate control. Current consensus, based largely on the RACE-II trial (1) suggests that a HR < 110 BPM is adequate (they compared HR < 80 vs HR 110 BPM).
Beta-blockers (eg metoprolol) and Calcium Channel Blockers (CCBs) (eg Diltiazem, Verapamil - see below) are suggested as first line therapy if considering rate controlling AF. Other drugs for rate control include Digoxin and Amiodarone (which can also Rhythm control)
Consideration for the individual patient will dictate choice of therapy, for example;
Calcium Channel Blockers
All CCBs aren't created equal. You have Dihydropyridines, which target systemic Ca channels and Non-Dihydropyridines which have variable effect on cardiac Ca channels.
The Dihydropyridines (eg amlodipine, nifedipine, nimodipine) are ineffectual in AF.
The Non-Dihydropyridines aren't created equal either. Briefly, you have Benzothiazepine (eg Dilatiazem) which have both cardiac and systemic effects and Phenylalkylamine (eg Verapamil) which are mostly cardiac. Therefore, for the saggy blood pressured patient, Verapamil is preferred if you want to use a CCB.
Digoxin
Digoxin is a very safe drug in the acute setting, and often not that useful. Let me explain.
Digoxin inhibits Na/K ATPase (mostly selective for myocardium) causing ↑ contractility. It also ↑ vagal efferent activity to the heart ie ↓ chronotropy. This is how it helps in AF. The problem with digoxin are 3-fold;
1. Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362(15):1363-73.
Beta-blockers (eg metoprolol) and Calcium Channel Blockers (CCBs) (eg Diltiazem, Verapamil - see below) are suggested as first line therapy if considering rate controlling AF. Other drugs for rate control include Digoxin and Amiodarone (which can also Rhythm control)
Consideration for the individual patient will dictate choice of therapy, for example;
- Beta blockers aren't ideal in patients with reactive airway disease, or haemodynamic instability
- Beta blockers are preferred in thyroid related AF and AF complicating ACS (if not unstable)
- CCBs and Digoxin should not be given to patients with AF AND pre-excitation syndrome (they'll develop VF from uninhibited transmission of fibrillating electrical activity to the ventricle via accessory pathways (use Flecanide or Amiodarone instead)
- Amiodarone is the drug of choice for severe LV dysfunction (followed by digoxin) and therefore often the first choice in critically ill patients
Calcium Channel Blockers
All CCBs aren't created equal. You have Dihydropyridines, which target systemic Ca channels and Non-Dihydropyridines which have variable effect on cardiac Ca channels.
The Dihydropyridines (eg amlodipine, nifedipine, nimodipine) are ineffectual in AF.
The Non-Dihydropyridines aren't created equal either. Briefly, you have Benzothiazepine (eg Dilatiazem) which have both cardiac and systemic effects and Phenylalkylamine (eg Verapamil) which are mostly cardiac. Therefore, for the saggy blood pressured patient, Verapamil is preferred if you want to use a CCB.
Digoxin
Digoxin is a very safe drug in the acute setting, and often not that useful. Let me explain.
Digoxin inhibits Na/K ATPase (mostly selective for myocardium) causing ↑ contractility. It also ↑ vagal efferent activity to the heart ie ↓ chronotropy. This is how it helps in AF. The problem with digoxin are 3-fold;
- Time of onset is HOURS
- It doesn't work if there is too much sympathetic activity eg exercise, sepsis, drugs or surgery. Having said that, it does work well and safely for the sedentary (and lets face it, the largest population with AF are > 85 years old). So choose your patients wisely.
- Has no role in preventing further episodes of AF, so not useful to use in the long term (unless given for heart failure, which is also debatable)
1. Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362(15):1363-73.
Rhythm Control
Rhythm control is contraindicated for patients in AF for > 48hrs. Some small non-randomised trials are starting to emerge that suggest a trend in better outcomes with shorter cut offs. These are, however, trends. If the time of onset is unknown or > 48hrs then it is imperative that a TOE is performed to ensure that there is no intra-atrial clot.
The main question of rhythm control is whether you use drugs or electricity.
Electricity
Electricity has its benefits in that it is around 90% successful, which is why it is the first line in an unstable patient. Of course the risks, aside from pain, burns, arrythmias and not reverting include the risks associated with sedation for the procedure.
Drugs
Amiodarone (Class III) and Flecanide (Class Ic) have been implicated in rhythm control for AF. These have been so successful that cardiologists have been known to supply patients with pAF with a "Pill-in-the-pocket" approach to recurrence of pAF. This involves taking a beta blocker after symptom onset, then take flecanide (~300mg - check local guidelines). This works around 80% of the time (i was unable to find mean time to reversion). A beta blocker pre-med is given to prevent 1:1 ventricular conduction of flutter if the reversion is not successful. Note that flecanide should only be used with a known normal LVEF (Class I drugs have fallen out of fashion as they have shown a trend towards higher mortality (this has not been explored further in any great detail in the literature).
The main question of rhythm control is whether you use drugs or electricity.
Electricity
Electricity has its benefits in that it is around 90% successful, which is why it is the first line in an unstable patient. Of course the risks, aside from pain, burns, arrythmias and not reverting include the risks associated with sedation for the procedure.
Drugs
Amiodarone (Class III) and Flecanide (Class Ic) have been implicated in rhythm control for AF. These have been so successful that cardiologists have been known to supply patients with pAF with a "Pill-in-the-pocket" approach to recurrence of pAF. This involves taking a beta blocker after symptom onset, then take flecanide (~300mg - check local guidelines). This works around 80% of the time (i was unable to find mean time to reversion). A beta blocker pre-med is given to prevent 1:1 ventricular conduction of flutter if the reversion is not successful. Note that flecanide should only be used with a known normal LVEF (Class I drugs have fallen out of fashion as they have shown a trend towards higher mortality (this has not been explored further in any great detail in the literature).
Placebo
 | Perhaps the most important and often forgotten intervention is no intervention at all. As Brian's study (click on the image to download the paper) suggests, of the 35 patients recruited, 63% reverted within 48hrs without intervention, no adverse events occurred in either group and 9% returned within 30 days with recurrence. |
3. Anticoagulation
As has been explained, there is a statistically significant risk of stroke from AF (both NVAF and VAF).
VAF patients routinely get anti-coagulated.
NVAF patients need to be risk stratified.
VAF patients routinely get anti-coagulated.
NVAF patients need to be risk stratified.
| Risk Stratification in NVAF: CHA2DS2-VASc C +1 CHF H +1 HTN A +2: >74 D +1 Diabetes S +2 Stroke/TIA/Thromboembolism V +1 Vascular Hx A +1 Age 65-74 Sc +1 Female Anyone that scores 2 or more should be anti-coagulated (a score of 2 = 2.2% risk of stroke per year) |  The paper derivation for CHADS2-VASc 2009, n=1084 Primary Outcome: Stroke |
Drugs for Anticoagulation
5 years ago it was simple. Warfarin with bridging heparin would invariably be the answer. Now that novel oral anticoagulants (NOACs) have hit the market, the evidence is playing catch up. And remember - even if you cardiovert, you need to anti-coagulate if they meet risk stratification criteria.
What exists
Anti Thrombin: Heparin
Anti Vit K: warfarin
Anti Xa: Apixaban, Rivaroxaban
Anti IIa: Dabigatran
Some salient points about NOACs
What exists
Anti Thrombin: Heparin
Anti Vit K: warfarin
Anti Xa: Apixaban, Rivaroxaban
Anti IIa: Dabigatran
Some salient points about NOACs
- Dabigatran is dialysable but also causes stomach upsets (it needs an acidic environment to be absorbed)
- Rivaroxaban is a once daily dosing but is not dialysable
- There are currently no antidotes for any of the NOACS available in Australia
- All NOACs need to be renally adjusted
- efficacy against each other and warfarin are yet to be statistically convincing for better or worse
Maintenance of Sinus Rhythm
Both Amiodarone and Sotalol (Beta-blocker with Class III properties) are used to maintain sinus rhythm. Sotalol is preferred as its side effect profile is safer. Starting one of this medications is beyond the scope of this blog.
1. Medi C, Hankey GJ, Freedman SB. Atrial fibrillation. Med J Aust 2007;186:197-202.
1. Medi C, Hankey GJ, Freedman SB. Atrial fibrillation. Med J Aust 2007;186:197-202.
Intervention
Ablation therapy remains the cornerstone of interventional therapy if applicable.
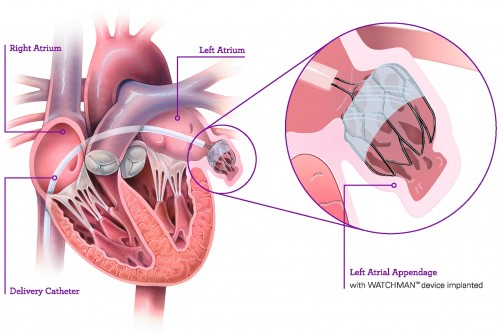
The Watchman's device (below) has been implicated in reducing stroke risk without anticoagulation in AF patients. Non randomised trials have shown that, combined with ablation, stroke risk is 0.5% per year (1)
1. Phillips, Karen P., Daniel T. Walker, and Julie A. Humphries. "Combined Catheter Ablation For Atrial Fibrillation And Watchman® Left Atrial Appendage Occlusion Procedures: Five-Year Experience".Journal of Arrhythmia 32.2 (2016): 119-126.
The Watchman's device (below) has been implicated in reducing stroke risk without anticoagulation in AF patients. Non randomised trials have shown that, combined with ablation, stroke risk is 0.5% per year (1)
1. Phillips, Karen P., Daniel T. Walker, and Julie A. Humphries. "Combined Catheter Ablation For Atrial Fibrillation And Watchman® Left Atrial Appendage Occlusion Procedures: Five-Year Experience".Journal of Arrhythmia 32.2 (2016): 119-126.
CASES TO TURN THE COGS
Case 1. The Incidental Finding
Therese is a 67yo female who went to her GP for a refill of her metformin. Routine examination revealed a new irregular heart rate without symptoms. Her ECG shows AF at a rate of 130 BPM and is referred to the Emergency Department for further management.
Key Features
Therese is stable.
Time of onset is unknown, so either a TOE or no shock unless she becomes unstable for this presentation.
No apparent history of PIRATEs
Proposed Management (there's more than one way to skin a cat!)
Workup includes TFTs and electrolytes (for what its worth)
Rate control with a beta blocker and assess Stroke risk and give a NOAC if needed.
Outpatient Echo and cardiology follow up is appropriate
Therese is a 67yo female who went to her GP for a refill of her metformin. Routine examination revealed a new irregular heart rate without symptoms. Her ECG shows AF at a rate of 130 BPM and is referred to the Emergency Department for further management.
Key Features
Therese is stable.
Time of onset is unknown, so either a TOE or no shock unless she becomes unstable for this presentation.
No apparent history of PIRATEs
Proposed Management (there's more than one way to skin a cat!)
Workup includes TFTs and electrolytes (for what its worth)
Rate control with a beta blocker and assess Stroke risk and give a NOAC if needed.
Outpatient Echo and cardiology follow up is appropriate
Case 2. The Footy Fan
Jeff is a 45yo male who turned up to work today as a call centre operator and felt a sudden onset of palpitations and feeling shaky. This has never happened before. The boss calls an ambulance and he arrives to you 1 hr later. He is otherwise well but admits to having a bender after his team won the croquette yesterday.
Key Features
Jeff is stable.
Time of onset is 1 hr ago so cardioversion is on the table.
He sounds like he has "Holiday Heart" according to the story.
Proposed Management (there's more than one way to skin a cat!)
A little diazepam for the withdrawal might help with the shaky symptoms.
Assuming there are no risks associated with having a procedural sedation, given the time of onset is known, cardioversion is one possibility.
Alternatively, given that 67% of Jeff's will revert in 48hrs, asking him to come back the next day fasted for a cardioversion may prevent the need for a procedural sedation yet stay within the 48hr windows for cardioversion if placebo hasn't worked.
Don't forget to assess need for anticoagulation.
Jeff is a 45yo male who turned up to work today as a call centre operator and felt a sudden onset of palpitations and feeling shaky. This has never happened before. The boss calls an ambulance and he arrives to you 1 hr later. He is otherwise well but admits to having a bender after his team won the croquette yesterday.
Key Features
Jeff is stable.
Time of onset is 1 hr ago so cardioversion is on the table.
He sounds like he has "Holiday Heart" according to the story.
Proposed Management (there's more than one way to skin a cat!)
A little diazepam for the withdrawal might help with the shaky symptoms.
Assuming there are no risks associated with having a procedural sedation, given the time of onset is known, cardioversion is one possibility.
Alternatively, given that 67% of Jeff's will revert in 48hrs, asking him to come back the next day fasted for a cardioversion may prevent the need for a procedural sedation yet stay within the 48hr windows for cardioversion if placebo hasn't worked.
Don't forget to assess need for anticoagulation.
Case 3. The Unlikely Presenter
Mary is a 62yo female brought in by ambulance with sudden onset chest pain, palpitations and presyncope (she's not sure which came first). She says it started 5 days ago but she has only really become dizzy tonight. She has been otherwise well recently. She admits to a history of refractory hypertension and poor compliance with her own health care. The ambulance crew noted she was in AF at a rate of 210-230BPM with a BP of 96/70. Her 12 lead shows rapid AF without lateral ST depression.
Key Features
For someone who's normally hypertensive (refractory no less), she got a saggy BP.
Plan
She's unstable, cardioversion is indicated despite having symptoms of AF > 48hrs. Don't forget to put the bed card in and refer the patient to an inpatient team.
Mary is a 62yo female brought in by ambulance with sudden onset chest pain, palpitations and presyncope (she's not sure which came first). She says it started 5 days ago but she has only really become dizzy tonight. She has been otherwise well recently. She admits to a history of refractory hypertension and poor compliance with her own health care. The ambulance crew noted she was in AF at a rate of 210-230BPM with a BP of 96/70. Her 12 lead shows rapid AF without lateral ST depression.
Key Features
For someone who's normally hypertensive (refractory no less), she got a saggy BP.
Plan
She's unstable, cardioversion is indicated despite having symptoms of AF > 48hrs. Don't forget to put the bed card in and refer the patient to an inpatient team.
Case 4. The VIP
Angus is a 78yo male with a history of hypertension, AMI/stents/CABG, DM and COPD (4 admissions last winter). His wife was concerned as he complained that his heart was racing and he had chest pain, "like the time i had my heart attack". He has had previous presentations with AF and is on warfarin and metoprolol. There is no history leading up to this. He is haemodynamically stable and a 12 lead ecg shows AF at a rate of 130BPM with non-specific ST & T wave changes.
Key Features
Angus is stable.
Time of onset is < 48hrs.
He has a history of AF and is on rate control medication. No other history of PIRATES.
Plan.
It would be suitable to ask Angus if or when his metoprolol is due and give him another oral dose. He's not far off the target of 110BPM for rate control. Of course, given his age, we will need to cross off all the PIRATES prior to discharge
Angus is a 78yo male with a history of hypertension, AMI/stents/CABG, DM and COPD (4 admissions last winter). His wife was concerned as he complained that his heart was racing and he had chest pain, "like the time i had my heart attack". He has had previous presentations with AF and is on warfarin and metoprolol. There is no history leading up to this. He is haemodynamically stable and a 12 lead ecg shows AF at a rate of 130BPM with non-specific ST & T wave changes.
Key Features
Angus is stable.
Time of onset is < 48hrs.
He has a history of AF and is on rate control medication. No other history of PIRATES.
Plan.
It would be suitable to ask Angus if or when his metoprolol is due and give him another oral dose. He's not far off the target of 110BPM for rate control. Of course, given his age, we will need to cross off all the PIRATES prior to discharge
 RSS Feed
RSS Feed