
 | Viet Tran 21yo female presents to DEM complaining of tightness in throat with associated crackling and swelling of the neck and without SOB. She had an uncomplicated home birth 18 hours ago (G9P9) without any significant past history. Obs are normal including Sat 99%RA RR12, oropharynx appears normal but she does appear to have mild diffuse swelling of the neck without focal tenderness or fluctuations. |
Describe the X-ray
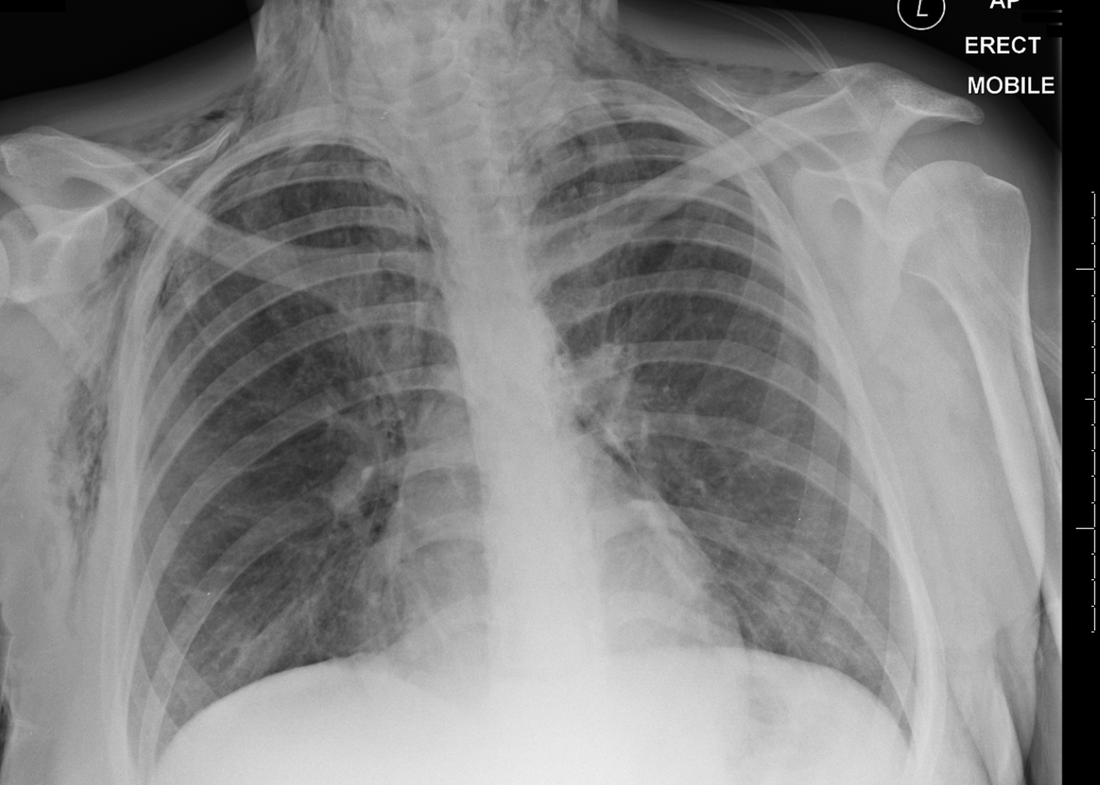
Under-penetrated slightly rotated erect AP chest x-ray
Mediastinum midline, lung markings to edge of thoracic cage, no obvious consolidation or suspicion for wedge infarct
Cardiothoracic ratio within normal limits
Cardiac silhouette better defined than expected with a suggestion of air dissecting the pericardium away from the heart (especially the left heart border)
Upper mediastinal contour on the left suggests air around heart confluent with upper mediastinum (again, more defined on the left mediastinal border)
Marked subcutaneous emphysema in the upper chest and neck
No direct evidence of boney pathology including rib fracture(s), no surrogate markers for rib fractures including rib crowding or deep sulcus (although the position is erect)
No obvious sub-diaphragmatic pathology
Top right area of the film appears to show oxygen tubing with an absence of ecg dots or other paraphenelia
Impression: Pneumomediastinum with extensive subcutaneous emphysema without an obvious cause. No evidence of pneumothorax.
Mediastinum midline, lung markings to edge of thoracic cage, no obvious consolidation or suspicion for wedge infarct
Cardiothoracic ratio within normal limits
Cardiac silhouette better defined than expected with a suggestion of air dissecting the pericardium away from the heart (especially the left heart border)
Upper mediastinal contour on the left suggests air around heart confluent with upper mediastinum (again, more defined on the left mediastinal border)
Marked subcutaneous emphysema in the upper chest and neck
No direct evidence of boney pathology including rib fracture(s), no surrogate markers for rib fractures including rib crowding or deep sulcus (although the position is erect)
No obvious sub-diaphragmatic pathology
Top right area of the film appears to show oxygen tubing with an absence of ecg dots or other paraphenelia
Impression: Pneumomediastinum with extensive subcutaneous emphysema without an obvious cause. No evidence of pneumothorax.
What is the Eponymous name for this pathology?
Hamman's Syndrome (1939) (1)
Primary pneumomediastinum & subsequent subcutaneous emphysema - often due to (but not limited to) labour, exacerbation of asthma, violent coughing but most commonly spontaneous (34% of all primary pneumomediastinums) (3)
Relating specifically to the peri-partum period, Hamman's syndrome occurs in approximalty 1 in 100,000 SVDs, more common in primips with a powerful 2nd stage and usually a delayed diagnosis.
Primary pneumomediastinum & subsequent subcutaneous emphysema - often due to (but not limited to) labour, exacerbation of asthma, violent coughing but most commonly spontaneous (34% of all primary pneumomediastinums) (3)
Relating specifically to the peri-partum period, Hamman's syndrome occurs in approximalty 1 in 100,000 SVDs, more common in primips with a powerful 2nd stage and usually a delayed diagnosis.
What is the Pathophysiology
Known as the Macklin Effect (2), raised intra-alveolar pressure can sometimes cause alveolar to rupture. Air subsequently escapes, tracking down bronchovascular sheaths towards the hilum and from there, mediastinal and subcutaneously.
40% of pneumomediastinum in blunt chest trauma is due to the Macklin effect - of course you dont want to miss more sinister pathology in this group (see below)
40% of pneumomediastinum in blunt chest trauma is due to the Macklin effect - of course you dont want to miss more sinister pathology in this group (see below)
What are your Differential Diagnosis?
In post-partum patients also think about Boerhaave’s syndrome, Amniotic fluid embolus, Pneumothorax, PE, MI and Mediastinitis
In blunt chest trauma also think about Tracheobronchial rupture, oesophageal rupture (Boerhaave's) or pneumothorax
In blunt chest trauma also think about Tracheobronchial rupture, oesophageal rupture (Boerhaave's) or pneumothorax
What is your management?
Hamman's syndrome has a relatively benign course (3), usually necessitates symptomatic management and avoidance of further investigations. Observation, symptomatic management and Oxygen are the mainstay of treatment.
Intervention is usually only required when there is an underlying lung condition (eg bullous emphysema) complicating the usual course of Hamman's syndrome. Said complications include pneumothorax, recurrence or further progression.
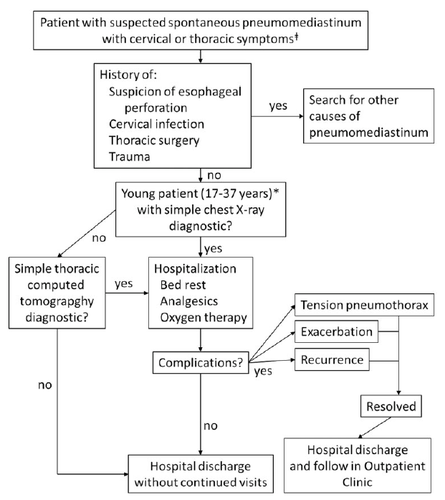
Walid et al (3) following a systematic review of (n=600 over 27 papers of variable quality) suggested the following algorithm:
Intervention is usually only required when there is an underlying lung condition (eg bullous emphysema) complicating the usual course of Hamman's syndrome. Said complications include pneumothorax, recurrence or further progression.
Walid et al (3) following a systematic review of (n=600 over 27 papers of variable quality) suggested the following algorithm:
References
- Hamman L. Spontaneous mediastinal emphysema. Bull Hopkins Hosp 1937; 64: 1–21.
- Macklin CC. Transport of air along sheaths of pulmonic blood vessels from alveoli to mediastinum: clinical impli- cations. Arch Intern Med 1939;64:913–26.
- Dajer-Fadel WL, Arguero-Sanchez R, Ibarra-Perez C, Navarro-Reynoso FP. Systematic review of spontaneous pneumomediastinum: A survey of 22 years' data. Asian Cardiovascular and Thoracic Annals. 2014 Sep 22;22(8):997–1002.
 RSS Feed
RSS Feed